💀 Facial Fractures — Otolaryngology Inpatient Coding Reference
📑 Table of Contents
- Anatomical Regions Covered
- 7th Character Rules — S02 Fracture Codes
- ICD-10-CM Code Families — Detailed Breakdown
- LeFort Fracture Classification
- ICD-10-PCS — Operative Repair
- MS-DRG Assignment
- Coding Scenarios
- Common CDI Queries
- External Cause Coding
- Adding Images — Guide
- Related Notes
Quick Orientation
Facial fractures in inpatient coding fall under ICD-10-CM Chapter 19 (S00-T88) — Injury, Poisoning, and Certain Other Consequences of External Causes. The 7th character is critical for every code in this family. Operative management maps to ICD-10-PCS and associated CPT codes. MS-DRGs 152-154 govern these cases.
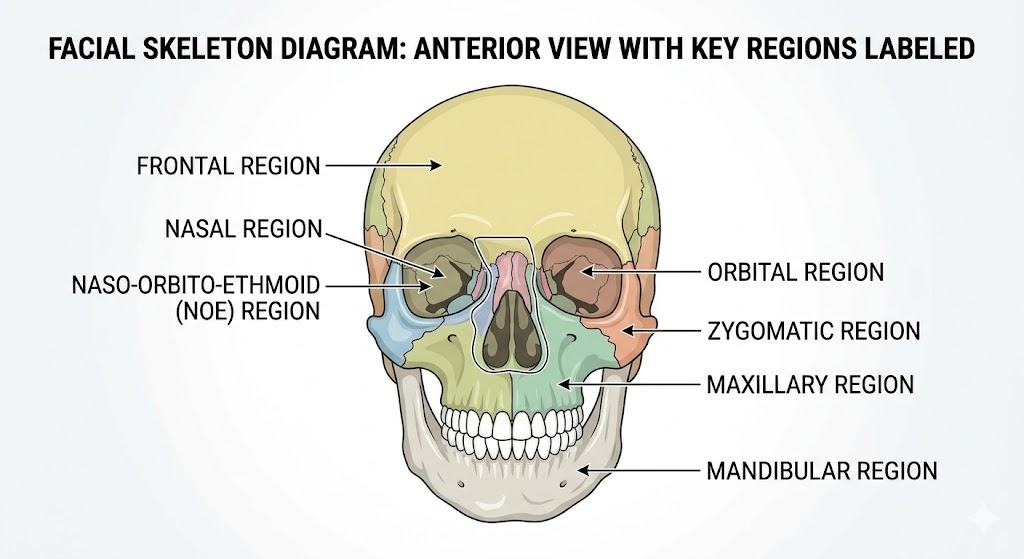
🗺️ Anatomical Regions Covered (Otolaryngology-Relevant)
| Region | Bones Involved | Clinical Significance |
|---|---|---|
| Frontal sinus / skull base | Frontal bone, anterior/posterior table | Intracranial involvement risk |
| Nasal bones | Nasal bones, nasal septum | Most common facial fracture |
| Naso-orbito-ethmoid (NOE) | Nasal, ethmoid, lacrimal, frontal process of maxilla | Telecanthus, CSF leak risk |
| Orbital | Orbital floor, medial/lateral walls, orbital rim | Entrapment, enophthalmos |
| Zygoma / Zygomatic arch | Zygomatic bone, zygomatic arch | Tripod/tetrapod fracture pattern |
| Maxilla (LeFort) | Maxilla, pterygoid plates, and variable other bones | Classified I/II/III by level |
| Mandible | Body, ramus, condyle, symphysis, alveolar | Most common jaw fracture site: body |
| Alveolar process | Maxillary or mandibular alveolar ridge | Dental/alveolar trauma |
| Palate | Hard palate | Often accompanies LeFort II/III |
Facial Anatomy
📋 7th Character Rules — S02 Fracture Codes
7th Character is Non-Negotiable
Every S02 fracture code requires a 7th character. Missing or incorrect 7th characters are a top claim denial driver for facial fracture encounters.
| 7th Character | Meaning | When to Use |
|---|---|---|
| A | Initial encounter | Active treatment — surgery, ED, first admission for fracture care |
| B | Initial encounter, open fracture | Active treatment of an open facial fracture |
| D | Subsequent encounter | Routine healing, follow-up, cast/splint check |
| G | Subsequent encounter, delayed healing | Healing slower than expected |
| K | Subsequent encounter, nonunion | Fracture failed to unite |
| S | Sequela | Condition arising as a result of prior healed fracture |
Inpatient 7th Character Tip
Inpatient admissions for fracture repair almost always use A (initial encounter). Use B only when documentation explicitly states the fracture is open (laceration communicating with fracture site, or penetrating wound). A laceration alone does not make a fracture “open.”
🦴 ICD-10-CM Code Families — Detailed Breakdown
S02.0 — Fracture of Vault of Skull / Frontal Bone
S02.0 — Frontal Bone Fractures
The frontal sinus and frontal bone are ENT and neurosurgery territory. Posterior table involvement triggers neurosurgery consult and potential intracranial complication codes.
| Code | Description |
|---|---|
| S02.0XXA | Fracture of vault of skull, initial encounter |
| S02.0XXB | Fracture of vault of skull, open, initial encounter |
| S02.0XXD | Fracture of vault of skull, subsequent encounter |
| S02.0XXK | Fracture of vault of skull, nonunion |
| S02.0XXS | Fracture of vault of skull, sequela |
Anterior vs. Posterior Table:
- Anterior table only: managed surgically by ENT/plastics; lower intracranial risk
- Posterior table: neurosurgery involvement; code also any associated intracranial injury (S06.-)
- Nasofrontal outflow tract involvement: document for surgical planning (affects DRG complexity)
Common associated codes:
- S09.90XA — Unspecified injury of head (if intracranial component not fully specified)
- G96.00 — CSF leak, unspecified (if dural tear)
S02.2 — Fracture of Nasal Bones
S02.2 — Nasal Fractures
Most common facial fracture. Simple nasal fractures are often treated in the ED or outpatient setting. Inpatient admission typically signals complexity: septal hematoma, septal fracture/dislocation, epistaxis requiring packing/intervention, or concomitant injuries.
| Code | Description |
|---|---|
| S02.2XXA | Fracture of nasal bones, initial encounter |
| S02.2XXB | Fracture of nasal bones, open, initial encounter |
| S02.2XXD | Fracture of nasal bones, subsequent encounter |
| S02.2XXK | Fracture of nasal bones, nonunion |
| S02.2XXS | Fracture of nasal bones, sequela |
Coding pearls:
- Nasal septal fracture is captured under S02.2— (no separate septal fracture code in ICD-10-CM)
- Septal hematoma = S09.90XA or consider S09.8XXA (other specified head injury)
- Epistaxis associated with nasal fracture: R04.0 — code as additional dx if clinically managed
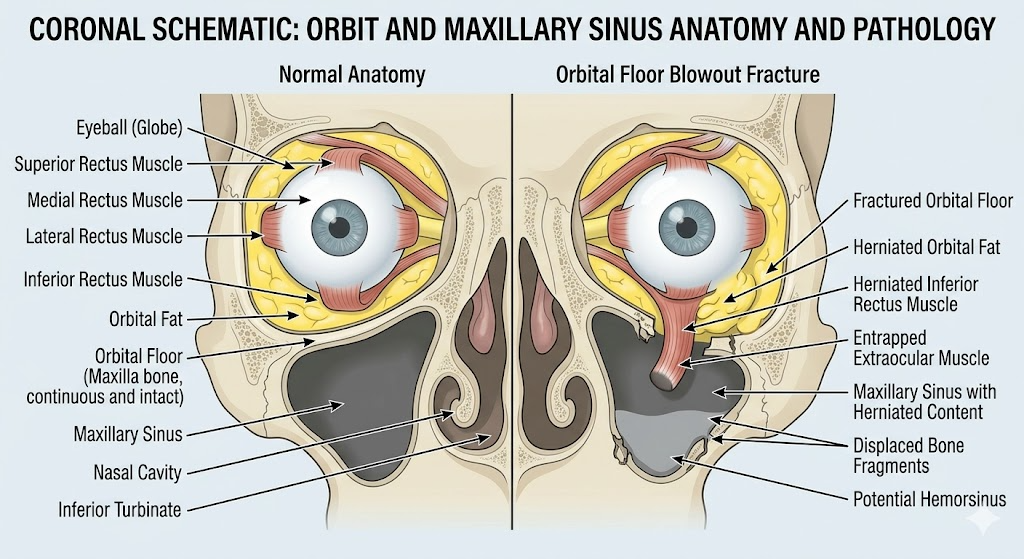
S02.3 — Fracture of Orbital Floor
S02.3 — Orbital Floor ("Blowout") Fractures
Classic blowout mechanism: direct force to globe → increased intraorbital pressure → floor fractures into maxillary sinus. Key clinical concern: inferior rectus entrapment, enophthalmos, diplopia.
| Code | Description |
|---|---|
| S02.3XXA | Fracture of orbital floor, initial encounter |
| S02.3XXB | Fracture of orbital floor, open, initial encounter |
| S02.3XXD | Fracture of orbital floor, subsequent encounter |
Coding pearls:
- Orbital floor fracture = S02.3, NOT S02.4 (which is malar/zygomatic)
- Medial orbital wall fracture → use S02.83- (other orbital fractures)
- Entrapment documented → add H50.9 (unspecified strabismus) or specific motility code
- Eye injury: code separately — S05.- for globe/orbital soft tissue injuries
- White-eyed blowout (pediatric trapdoor): emergent — document and code entrapment explicitly
Orbital Anatomy
S02.4 — Fractures of Malar, Maxillary, and Zygoma
S02.4 — Zygomatic/Malar Complex Fractures
Zygoma articulates at 4 points: frontozygomatic suture, zygomaticomaxillary buttress, infraorbital rim, and zygomatic arch. Classic “tripod” fracture disrupts 3 of these. Now more accurately called tetrapod or zygomaticomaxillary complex (ZMC) fracture.
| Code | Description |
|---|---|
| S02.400A | Malar fracture, unspecified side, initial encounter |
| S02.401A | Malar fracture, right side, initial encounter |
| S02.402A | Malar fracture, left side, initial encounter |
| S02.40AA | Maxillary fracture, unspecified side, initial encounter |
| S02.40BA | Maxillary fracture, right side, initial encounter |
| S02.40CA | Maxillary fracture, left side, initial encounter |
| S02.40DA | Zygomatic arch fracture, unspecified side, initial encounter |
| S02.40EA | Zygomatic arch fracture, right side, initial encounter |
| S02.40FA | Zygomatic arch fracture, left side, initial encounter |
| S02.411A | LeFort I fracture, right side, initial encounter |
| S02.412A | LeFort I fracture, left side, initial encounter |
| S02.42XA | LeFort II fracture, initial encounter |
NOTE
Laterality note: Malar and zygomatic arch codes are side-specific. Query provider if documentation says only “left” or “right” ZMC fracture without specifying malar vs. arch component.
S02.6 — Fractures of Mandible
S02.6 — Mandibular Fractures
Mandible is the most frequently fractured facial bone after the nasal bones. The body is the most common site. Condylar fractures are common in falls/MVAs. Bilateral condylar = high energy. Subcondylar vs. condylar head distinction matters clinically but codes similarly.
| Code | Description |
|---|---|
| S02.600A | Fracture of unspecified part of body of mandible, unspecified, initial encounter |
| S02.600B | Open fracture of unspecified part of body of mandible, initial encounter |
| S02.601A | Fracture of body of mandible, right side, initial encounter |
| S02.602A | Fracture of body of mandible, left side, initial encounter |
| S02.609A | Fracture of body of mandible, unspecified, initial encounter |
| S02.610A | Fracture of condylar process of mandible, unspecified, initial encounter |
| S02.611A | Fracture of condylar process, right mandible, initial encounter |
| S02.612A | Fracture of condylar process, left mandible, initial encounter |
| S02.619A | Fracture of condylar process, unspecified mandible, initial encounter |
| S02.620A | Fracture of subcondylar process of mandible, unspecified, initial encounter |
| S02.630A | Fracture of coronoid process of mandible, unspecified, initial encounter |
| S02.640A | Fracture of ramus of mandible, unspecified, initial encounter |
| S02.650A | Fracture of angle of mandible, unspecified, initial encounter |
| S02.670A | Fracture of alveolar process of mandible, unspecified, initial encounter |
Open vs. Closed Mandible Fracture:
- Mandibular body fractures through tooth-bearing areas are almost always open (communicate with oral cavity)
- Provider documentation must state “open” — do not assume from anatomy alone unless queried and confirmed
- Consider querying provider if fracture is through dentition and no open/closed designation documented
S02.8 — Other Fractures of Skull and Face
S02.8 — NOE, Orbital, and Other Specified Facial Fractures
This subcategory captures the complex fractures that don’t fit neatly into other categories, including naso-orbito-ethmoid (NOE) fractures and medial/lateral orbital wall fractures.
| Code | Description |
|---|---|
| S02.80XA | Other fracture of skull, initial encounter |
| S02.80XB | Other open fracture of skull, initial encounter |
| S02.81XA | Fracture of orbital roof, initial encounter |
| S02.82XA | Fracture of lateral orbital wall, initial encounter |
| S02.831A | Fracture of medial orbital wall, right side, initial encounter |
| S02.832A | Fracture of medial orbital wall, left side, initial encounter |
| S02.839A | Fracture of medial orbital wall, unspecified side, initial encounter |
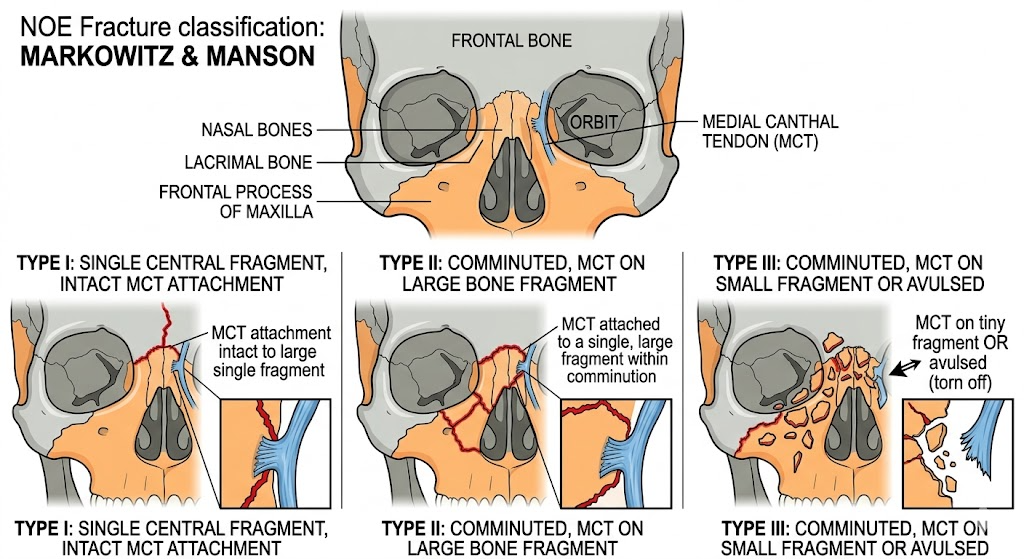
NOE Fractures:
- No single ICD-10-CM code for “naso-orbito-ethmoid fracture” as a unit
- Code each bone involved: nasal (S02.2), orbital medial wall (S02.83-), ethmoid component often captured with skull base codes
- NOE is a clinical classification (Markowitz Types I-III); map to anatomical ICD-10-CM codes
- Telecanthus, medial canthal tendon disruption → S01.01XA (open wound eyelid) if laceration present
NOE Fracture Classification
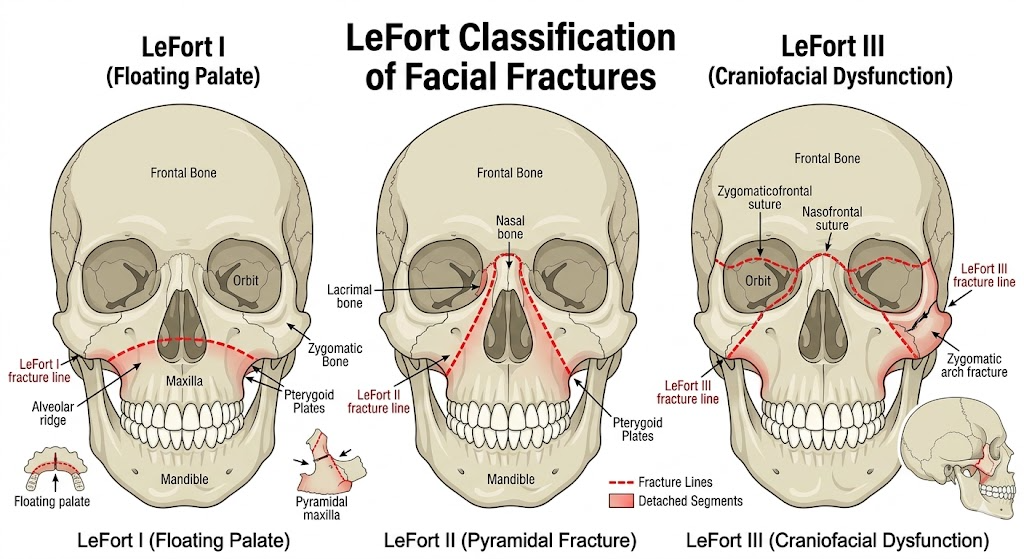
🏥 LeFort Fracture Classification — Deep Dive
LeFort Fractures — High Complexity, High DRG Impact
LeFort fractures are high-energy injuries. They almost always involve bilateral pterygoid plate fractures. Code bilateral involvement when documented.
| LeFort Level | Fracture Pattern | Key Bones | ICD-10-CM |
|---|---|---|---|
| LeFort I | Horizontal — above teeth, through maxillary sinuses | Maxilla, lower pterygoid plates | S02.411A / S02.412A |
| LeFort II | Pyramidal — through nasal bones, infraorbital rim, maxilla | Nasal, lacrimal, maxilla, pterygoid | S02.42XA |
| LeFort III | Craniofacial dysjunction — separates midface from skull | Zygomatic arches, orbital walls, nasal, ethmoid | S02.411A + S02.412A (bilateral if applicable) |
LeFort III Coding Challenge
ICD-10-CM does not have a standalone LeFort III code. LeFort III requires coding the component fractures: bilateral zygomatic arch, orbital walls, nasal bones, and involvement of other bones per documentation. Query provider for full extent of fracture.
LeFort Classification
🔧 ICD-10-PCS — Operative Facial Fracture Repair
PCS Root Operations for Facial Fractures
The two most common root operations are Reposition (reducing/aligning the fracture) and Replacement (when mesh/implant replaces bone). Fusion is used for mandibular condylar fractures managed with plate fixation at the joint.
Root Operation Logic
| Clinical Action | PCS Root Operation | Definition |
|---|---|---|
| Closed reduction (no incision) | Reposition (S) | Moving displaced body part back to normal position |
| ORIF (open incision, hardware) | Reposition (S) | Still reposition — the fixation device character captures the hardware |
| Titanium mesh/implant replacing bone | Replacement (R) | Biological/synthetic substitute replaces body part |
| Arch bars, MMF (maxillomandibular fixation) | Reposition (S) | External fixation device character |
PCS Body Part Values — Head and Facial Bones (0N)
| Body Part | PCS Value |
|---|---|
| Frontal Bone | B |
| Nasal Bone | N |
| Ethmoid Bone, Right | C |
| Ethmoid Bone, Left | D |
| Lacrimal Bone, Right | J |
| Lacrimal Bone, Left | K |
| Palatine Bone, Right | L |
| Palatine Bone, Left | M |
| Zygomatic Bone, Right | N |
| Zygomatic Bone, Left | P |
| Orbit, Right | Q |
| Orbit, Left | R |
| Maxilla | T |
| Mandible, Right | V |
| Mandible, Left | W |
| Facial Bone | X |
Device Character Values (Facial Fracture Repairs)
| Device | PCS Character |
|---|---|
| No device (closed reduction, no hardware) | Z |
| Internal fixation device (plates, screws) | 4 |
| External fixation device (arch bars, MMF, halo) | 5 |
| Synthetic substitute (mesh, implant) | J |
| Autologous tissue substitute (bone graft) | 7 |
Sample PCS Codes
| Procedure | PCS Code | Breakdown |
|---|---|---|
| ORIF right orbital floor, open, internal fixation | 0NRQO4Z | 0N-Reposition, R-Orbit Right, 0-Open, 4-Internal fix, Z-No qualifier |
| ORIF mandible left, open, plate and screw | 0NSW04Z | 0N-Reposition, W-Mandible Left, 0-Open, 4-Internal fix, Z-No qualifier |
| Closed reduction nasal fracture | 0NSNXZZ | 0N-Reposition, N-Nasal, X-External, Z-No device, Z-No qualifier |
| Maxillomandibular fixation (arch bars) | 0NSTX5Z | 0N-Reposition, T-Maxilla, X-External, 5-External fix, Z-No qualifier |
| Orbital floor implant (mesh) | 0NRQ0JZ | 0N-Replacement, Q-Orbit Right, 0-Open, J-Synthetic substitute, Z-No qualifier |
PCS Precision Points
- ORIF is still Reposition, not Repair — the root operation is determined by objective (moving bone back), not the fixation used
- Code each bone separately if multiple bones have ORIF performed
- Arch bars alone (no open incision) = External approach
- If bone graft taken from another site, code the Excision of the donor site separately
📊 MS-DRG Assignment — Facial Fractures
| MS-DRG | Title | Notes |
|---|---|---|
| 152 | Cranial/Facial Procedures W MCC | Complex facial fracture OR repair w/ major complication/comorbidity |
| 153 | Cranial/Facial Procedures W CC | Facial fracture repair w/ complication/comorbidity |
| 154 | Cranial/Facial Procedures W/O CC/MCC | Uncomplicated facial fracture repair |
Also possible depending on management:
| MS-DRG | Title | Notes |
|---|---|---|
| 157 | Dental and Oral Diseases W MCC | Mandibular fractures with dental focus, MCC present |
| 158 | Dental and Oral Diseases W CC | Mandibular fractures, CC present |
| 159 | Dental and Oral Diseases W/O CC/MCC | Simple mandibular fracture |
DRG Optimization
Capture all comorbidities and complications accurately. Common CCs/MCCs that elevate facial fracture DRGs:
- Acute blood loss anemia (D62) → CC
- CSF leak (G96.00) → MCC
- Aspiration pneumonia (J69.0) → MCC
- Traumatic intracranial hemorrhage (S06.-) → MCC
- Orbital cellulitis (H05.01-) → CC
- Acute respiratory failure (J96.00) → MCC
📌 Coding Scenarios — High-Yield Clinical Situations
Scenario 1: Isolated Nasal Fracture, Closed Reduction in OR
- PDX: S02.2XXA — Fracture of nasal bones, initial encounter
- PCS: 0NSNXZZ — Reposition nasal bone, external approach
- External cause: Code mechanism (MVA, assault, sports, etc.)
- DRG: Likely 154 (no CC/MCC)
Scenario 2: ZMC Fracture with ORIF, Orbital Floor Reconstruction with Mesh
- PDX: S02.401A — Malar fracture, right side (or left)
- Additional dx: S02.3XXA — Orbital floor fracture (if concurrent)
- PCS 1: 0NSN04Z — Reposition zygomatic bone, open, internal fixation
- PCS 2: 0NRQ0JZ — Replacement right orbit, open, synthetic substitute (mesh)
- DRG: 152 or 153 depending on CC/MCC
Scenario 3: Panfacial Fracture (LeFort III + Mandible + NOE)
- PDX: S02.42XA (LeFort II component) + multiple additional fracture codes
- Code all: Bilateral zygomatic arches, orbital walls, nasal, mandible, alveolar
- PCS: Multiple Reposition codes, one per operative bone with ORIF
- DRG: 152 (almost certainly MCC present in panfacial)
- Query: Provider for open vs. closed designation, all bones with hardware, graft use
Scenario 4: Mandibular Fracture, MMF (Arch Bars), No ORIF
- PDX: S02.601A or S02.602A — Fracture of body, right or left mandible
- PCS: 0NSTX5Z — Reposition maxilla, external fixation (arch bars applied to both jaws — may need bilateral coding)
- DRG: 154 or 159 depending on grouper behavior
Scenario 5: Orbital Roof Fracture with Intracranial Extension
- PDX: S02.81XA — Fracture of orbital roof
- Additional: S06.- — Intracranial injury if documented
- Consults: Neurosurgery involvement → code any neurosurgical procedure separately
- DRG: 52 or 53 (Intracranial Vascular Procedures) or 154 depending on neurosurgical intervention
🔗 External Cause Coding (Required)
External Cause Codes Are Required
Facial fractures require external cause coding. These do NOT drive DRG but are required for complete coding and trauma registry.
| External Cause Category | Code Range | Examples |
|---|---|---|
| Motor vehicle accident | V20-V79 | MVA most common mechanism |
| Assault | X92-Y09 | Interpersonal violence |
| Fall | W00-W19 | Ground-level fall |
| Sports/recreation | W21-W31, Y93 | Contact sports, cycling |
| Place of occurrence | Y93.- | Where injury happened |
| Activity | Y93.- | What patient was doing |
| Patient status | Y99.- | Civilian, military, leisure |
❓ Common Queries for Facial Fracture Encounters
Clinical Documentation Improvement (CDI) Queries
Use these as a guide for querying providers when documentation is incomplete.
- “The operative report documents a fracture through the tooth-bearing segment of the mandible with exposure of the fracture site intraorally. Can you clarify whether this is an open or closed fracture?”
- “Documentation describes a LeFort II fracture. Can you confirm whether there is also a LeFort III component (craniofacial dysjunction) or if this is isolated LeFort II?”
- “There is documentation of enophthalmos and diplopia post-orbital floor repair. Is this a complication of the fracture or the surgical repair? Is treatment required?”
- “The patient sustained concurrent nasal, ethmoid, and medial orbital wall fractures. Can you confirm whether this represents a naso-orbito-ethmoid (NOE) fracture and classify by Markowitz type?”
- “A bone graft was harvested from the calvarium. Can you document the donor site and confirm the graft type (autologous, split-thickness, etc.)?”
- “Post-operatively, the patient developed altered mental status. Can you clarify whether this represents a medication side effect, intracranial complication, or unrelated condition?”