Laryngeal Anatomy — Comprehensive Reference
The Three Anatomical Zones
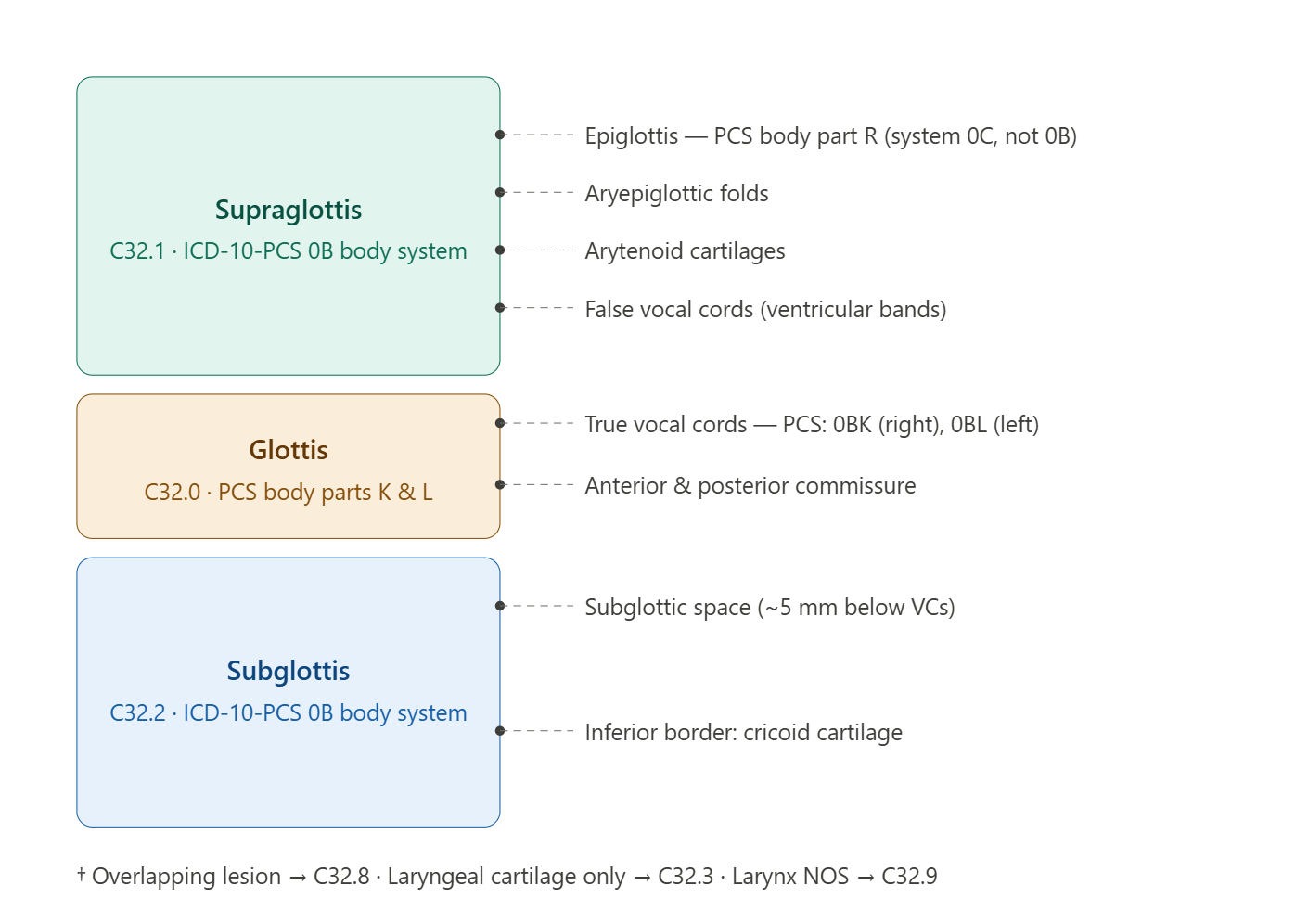
The larynx is divided into three zones, and zone specificity is required for neoplasm coding under category C32.A lesion that does not clearly fall within a single zone defaults to C32.8 (overlapping) or C32.9 (unspecified) — resist the urge to assign a specific zone code without clear documentation.
supraglottis (C32.1) extends from the tip of the epiglottis down to (but not including) the true vocal cords. Its subsites are the epiglottis (both the suprahyoid and infrahyoid portions), the aryepiglottic folds (laryngeal surface), the arytenoid cartilages, and the false vocal cords (ventricular bands). The supraglottis has rich lymphatic drainage, which is why supraglottic carcinomas often present with nodal disease.
glottis (C32.0) includes the true vocal cords, the anterior commissure, and the posterior commissure. It has poor lymphatic drainage — a clinically important fact because glottic carcinomas tend to stay localized longer, improving prognosis. For coding, “glottic” and “vocal cord” are generally synonymous unless the provider specifies a subglottic or supraglottic extension.
Subglottis (C32.2) begins approximately 5 mm below the free margin of the true vocal cords and extends to the inferior border of the cricoid cartilage. Subglottic primaries are the least common of the three and carry a poorer prognosis due to delayed presentation.
ICD-10-CM at a Glance
For neoplasms, the C32 category is entirely site-specific:
| Code | Description | Key note |
|---|---|---|
| C32.0 | Glottis | True VCs, commissures |
| C32.1 | Supraglottis | Includes epiglottis |
| C32.2 | Subglottis | Below VCs to cricoid |
| C32.3 | Laryngeal cartilage | Thyroid, cricoid, arytenoid, epiglottic cartilage as primary |
| C32.8 | Overlapping lesion | Spans two or more contiguous subsites |
| C32.9 | Larynx, unspecified | Use only when documentation is truly inadequate |
D02.0 covers carcinoma in situ of the larynx (including the epiglottis suprahyoid portion). **D14.**1 covers benign neoplasms of the larynx.
For non-neoplastic conditions, category J38 is the workhorse:
J38.0- covers vocal cord and laryngeal paralysis, with important specificity: J38.01 (unilateral) vs. J38.02 (bilateral). If the record simply says “vocal cord paralysis” without laterality, query before defaulting to J38.00. J38.1 is polyps, J38.2 is nodules, J38.3 covers a broad group including leukoplakia, granuloma, and cellulitis of the vocal cords. J38.4 is laryngeal edema, J38.5 is laryngeal spasm (including laryngismus stridulus), and J38.6 is stenosis.
ICD-10-PCS: The Critical 0B vs. 0C Distinction
This is the most common laryngeal PCS coding trap. The body systems split as follows:
Respiratory System (0B) contains the larynx and vocal cords:
- Body part J = Larynx (the organ as a whole)
- Body part K = Vocal Cord, Right
- Body part L = Vocal Cord, Left
Mouth and Throat (0C) contains the epiglottis:
- Body part R = Epiglottis
A biopsy of a vocal cord (0BBK8ZX) and a biopsy of the epiglottis (0BCR8ZX) land in completely different body system tables. If you see a direct laryngoscopy with biopsy of an epiglottic lesion, the root table is 0C, not 0B. Always check the operative report for exactly where the biopsy was taken.
Common Laryngeal Procedure Coding Notes
Diagnostic laryngoscopy — Inspection (J) of the Larynx, approach 8 (Via Natural or Artificial Opening Endoscopic): 0BJJ8ZZ. A flexible fiberoptic laryngoscopy in the office would use the same root operation but confirm approach documentation.
Microlaryngoscopy with excision (vocal cord polyp, nodule, cyst, papilloma) — Excision (B), Body part K or L, approach 8. Add the qualifier X for diagnostic (biopsy). A bilateral procedure on both cords = two separate codes.
Total laryngectomy — Resection (T) of Larynx (J), approach 0 (Open): 0BTJ0ZZ.
Partial laryngectomy — Excision (B) of Larynx (J), approach 0 (Open): 0BBJ0ZZ.
Vocal cord injection (for augmentation with collagen, fat, or similar material) — Supplement (U), body part K or L, approach 8.
Botulinum toxin injection into the larynx (for spasmodic dysphonia) — this codes to the Administration section (3E0), not Medical and Surgical. The substance character is Toxin (C) and the site is the Muscle body system.
Laryngeal dilation (for stenosis) — Dilation (7) of Larynx (J), with approach and device characters depending on whether a stent is left in place.
Coding Pearls
Epiglottis laterality doesn’t exist — the epiglottis is a single midline structure, so there is no right/left distinction for PCS body part R. Vocal cords, however, require right (K) vs. left (L) specificity, and bilateral procedures need two codes.
“Suprahyoid” vs. “infrahyoid” epiglottis — both portions code to C32.1 for malignant neoplasms. The distinction matters clinically (suprahyoid is above the hyoid bone and has different lymphatic patterns) but does not create a separate code.
Laryngeal cartilage fracture — codes to S12.8- (fracture of other specified cervical vertebrae)? No — actually to S19.8- or the specific injury codes for the neck structures. Query your encoder for the most current valid code since this is an uncommon fracture with coding nuances.
Voice changes (dysphonia) as a symptom — R49.0 (Dysphonia) is appropriate when it’s the presenting symptom without a confirmed underlying cause. Once a cause is coded (e.g., J38.0 for paralysis), the symptom code is generally omitted per ICD-10-CM guideline I.C.18.
Radiation laryngitis — if a patient has laryngitis documented as a consequence of radiation therapy, assign the appropriate J38 code plus an adverse effect code from the T-code table (T66-T78 range) with sequencing per the adverse effect guideline.
The larynx is a complex musculocartilaginous structure located in the anterior midline of the neck at the level of cervical vertebrae C3-C6 in adults. It serves three primary biological functions:
- Airway protection — prevents aspiration of food and liquid into the tracheobronchial tree during swallowing via coordinated sphincteric closure
- Phonation — produces voice through controlled vibration of the true vocal cords
- Respiration — maintains a patent airway and regulates airflow during breathing and Valsalva maneuvers
From a coding and surgical standpoint, precise knowledge of laryngeal anatomy is essential because ICD-10-CM, ICD-10-PCS, and CPT codes are highly site-specific within the larynx. A malignancy of the glottis (C32.0) is coded and staged entirely differently from a supraglottic malignancy (C32.1), and surgical approach, reconstruction, and DRG assignment all follow accordingly.
Topographic Location & Relationships
The larynx is bounded:
- Superiorly — by the hyoid bone and base of tongue (hypopharynx)
- Inferiorly — by the trachea (continuous at the inferior border of the cricoid cartilage)
- Anteriorly — by the strap muscles (sternohyoid, sternothyroid, thyrohyoid) and skin of the anterior neck
- Posteriorly — by the hypopharynx and esophageal inlet
- Laterally — by the piriform sinuses (bilateral recesses of the hypopharynx)
The laryngeal inlet (aditus laryngis) faces posterosuperiorly and is bounded by the epiglottis anteriorly, aryepiglottic folds laterally, and the interarytenoid space posteriorly.
Laryngeal Subsites — Clinical & Coding Divisions
The larynx is divided into three major anatomical and oncologic subsites. This division is universally used in ICD-10-CM coding, TNM staging, and surgical planning.
1. Supraglottis
The supraglottis encompasses all laryngeal structures above the level of the true vocal cords, specifically above the lateral margin of the laryngeal ventricle.
Structures included:
- Epiglottis (both lingual/anterior surface and laryngeal/posterior surface)
- Aryepiglottic folds
- Arytenoids (the cartilaginous prominences posteriorly)
- False vocal cords (ventricular folds / vestibular folds)
- Laryngeal ventricles (the space between the false and true vocal cords — also called the sinus of Morgagni)
Clinical significance:
- Supraglottic cancers often present late because the supraglottis is a relatively silent area — patients may not develop hoarseness (a hallmark of glottic disease) until there is inferior extension to the true cords
- Rich lymphatic drainage bilaterally → supraglottic cancers have a high rate of cervical lymph node metastasis (up to 50% at presentation)
- Supraglottic laryngectomy (horizontal partial laryngectomy) removes structures above the true cords while preserving voice
- Supraglottitis (formerly “epiglottitis”) is a potentially life-threatening infection of these structures
ICD-10-CM Coding:
- C32.1 — Malignant neoplasm of supraglottis
- J04.30 / J04.31 — Supraglottitis without/with obstruction
- J38.4 — Edema of larynx (can affect supraglottis)
2. Glottis
The glottis is the central functional unit of the larynx, defined as the true vocal cords and the area immediately adjacent, including the anterior and posterior commissures. It spans approximately 1 cm inferiorly below the free edge of the true vocal cord (per AJCC definition).
Structures included:
- True vocal cords (vocal folds) — right and left
- Anterior commissure — the point where both vocal cords meet anteriorly at the thyroid cartilage
- Posterior commissure — the interarytenoid space between the two vocal cord bodies posteriorly
True Vocal Cord Microanatomy:
The true vocal cord is a layered structure critical to voice production. From superficial to deep:
| Layer | Structure | Clinical Relevance |
|---|---|---|
| 1 | Stratified squamous epithelium | Mucosal surface; site of leukoplakia, CIS, early SCC |
| 2 | Superficial lamina propria (Reinke’s space) | Loose gelatinous layer; site of Reinke’s edema/polypoid corditis |
| 3 | Intermediate lamina propria | Elastic fiber layer; forms part of the vocal ligament |
| 4 | Deep lamina propria | Collagen fiber layer; completes the vocal ligament |
| 5 | Vocalis muscle (thyroarytenoid) | Intrinsic muscle; body of the cord |
Reinke’s space is of particular surgical importance — subepithelial procedures (microlaryngoscopy with submucosal resection, CPT 31545/31546) are designed to preserve the vocal ligament while evacuating pathological contents of this space.
Clinical significance:
- Glottic cancers present early due to dysphonia — even a small lesion disrupts the mucosal wave and causes hoarseness
- Sparse lymphatic supply at the glottis → low rate of nodal metastasis at presentation (unlike supraglottis)
- Excellent prognosis for early-stage (T1, T2) glottic cancers treated with radiation or laser cordectomy
- Vocal cord paralysis (J38.01/J38.02) most commonly reflects glottic-level dysfunction but the etiology is often at the level of the recurrent laryngeal nerve
ICD-10-CM Coding:
- C32.0 — Malignant neoplasm of glottis
- D02.0 — Carcinoma in situ of larynx (often glottic)
- J38.1 — Polyp of vocal cord and larynx
- J38.2 — Nodules of vocal cords
- J38.3 — Other diseases of vocal cords (leukoplakia, dysplasia, granuloma)
- J38.00 / J38.01 / J38.02 — Vocal cord paralysis
3. Subglottis
The subglottis extends from the inferior margin of the glottis (approximately 1 cm below the free edge of the true vocal cord) to the inferior border of the cricoid cartilage, where it transitions into the trachea.
Structures included:
- Subglottic mucosa and submucosa
- Inner surface of the cricoid cartilage ring (the only complete cartilaginous ring in the airway)
- Conus elasticus (the fibrous membrane connecting the thyroid and cricoid cartilages, continuous superiorly with the vocal ligament)
Clinical significance:
- Subglottic cancers are rare (< 5% of laryngeal cancers) but aggressive — the subglottis is a confined space, and tumors rapidly invade the cricoid cartilage or extend inferiorly to the trachea
- Subglottic stenosis (J38.6) is a common complication of prolonged intubation, tracheostomy, granulomatosis with polyangiitis (formerly Wegener’s), or prior surgery
- The subglottis is the narrowest part of the pediatric airway (at the level of the cricoid) — critical in pediatric airway management and a common site for subglottic hemangioma in infants
- Access for surgical intervention is limited; most procedures require endoscopic or open approaches through the cricothyroid or cricotracheotomy
ICD-10-CM Coding:
- C32.2 — Malignant neoplasm of subglottis
- J38.6 — Stenosis of larynx
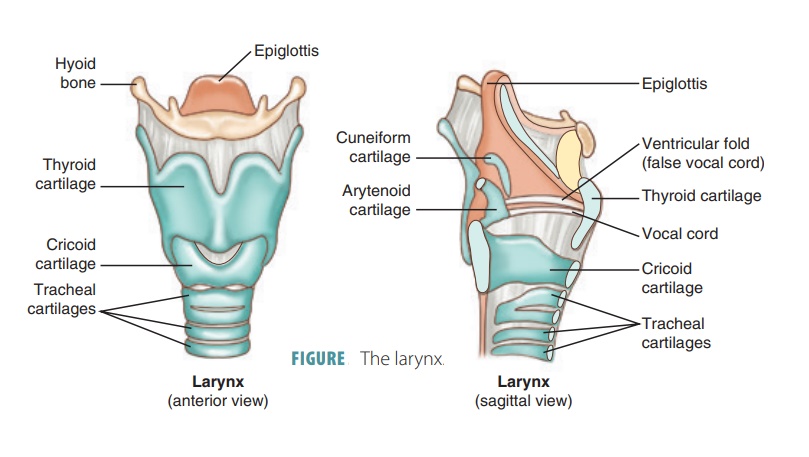
Laryngeal Cartilages
The laryngeal skeleton consists of nine cartilages — three paired and three unpaired.
Unpaired Cartilages
| Cartilage | Description | Clinical Notes |
|---|---|---|
| Thyroid cartilage | Largest laryngeal cartilage; two laminae fused anteriorly at the laryngeal prominence (Adam’s apple); angle is more acute in males (~90°) than females (~120°), explaining the more prominent Adam’s apple in men | The external perichondrium is a barrier to tumor spread; thyroid cartilage invasion upgrades laryngeal cancer to T4a (ICD-10 staging implication) |
| Cricoid cartilage | Signet ring-shaped; only complete cartilaginous ring in the entire airway; forms the inferior border of the larynx and articulates with the thyroid cartilage anterolaterally and the arytenoids posteriorly | Cricoid fracture in trauma is a surgical emergency; cricoid pressure (Sellick maneuver) used during rapid sequence intubation |
| Epiglottis | Leaf-shaped elastic fibrocartilage attached inferiorly to the thyroid cartilage at the petiole (stem); the superior free edge is the most visible structure at laryngoscopy | The vallecula (space between epiglottis and tongue base) is a common site for foreign body lodgment; the lingual surface of the epiglottis drains to the pre-epiglottic space, a critical anatomical plane in supraglottic surgery |
Paired Cartilages
| Cartilage | Description | Clinical Notes |
|---|---|---|
| Arytenoid cartilages | Pyramidal-shaped; sit atop the posterior cricoid plate; the vocal process projects anteriorly (attachment point of the vocal cord) and the muscular process projects laterally/posteriorly (attachment of intrinsic muscles); responsible for opening (abduction) and closing (adduction) the glottis | Arytenoid subluxation or dislocation can occur during intubation and causes unilateral vocal cord immobility; arytenoidectomy (CPT 31560/31561) is performed for bilateral vocal cord paralysis to improve the airway |
| Cuneiform cartilages | Small rod-shaped elastic cartilages embedded within the aryepiglottic folds superior to the corniculate cartilages | Appear as white nodular prominences on endoscopy within the aryepiglottic folds; minimal functional significance |
| Corniculate cartilages | Small cone-shaped elastic cartilages that cap the apices of the arytenoids | Visible on laryngoscopy as small nodular prominences at the posterior laryngeal inlet |
Laryngeal Joints
| Joint | Type | Function |
|---|---|---|
| Cricothyroid joint | Synovial joint between the inferior thyroid cornu and the lateral cricoid | Allows rocking/rotation that elongates and tenses the vocal cords (pitch change); innervated by the external branch of the superior laryngeal nerve |
| Cricoarytenoid joint | Synovial saddle joint between the base of the arytenoid and the superior surface of the posterior cricoid plate | Allows gliding and rotation of the arytenoid, controlling vocal cord abduction and adduction; arthritis or ankylosis here mimics vocal cord paralysis |
Intrinsic Muscles of the Larynx
All intrinsic muscles are innervated by the recurrent laryngeal nerve (RLN) except the cricothyroid, which is innervated by the external branch of the superior laryngeal nerve (eSLN).
| Muscle | Origin → Insertion | Action | Nerve |
|---|---|---|---|
| Posterior cricoarytenoid (PCA) | Posterior cricoid plate → muscular process of arytenoid | Sole abductor of the vocal cord; opens the glottis | RLN |
| Lateral cricoarytenoid (LCA) | Lateral cricoid arch → muscular process of arytenoid | Adducts the vocal cord (closes the glottis) | RLN |
| Transverse arytenoid (interarytenoid) | One arytenoid → opposite arytenoid | Adducts the posterior glottis (closes posterior commissure) | RLN (bilateral innervation) |
| Oblique arytenoid | Muscular process of one arytenoid → apex of opposite | Assists adduction; continuation forms the aryepiglottic muscle | RLN |
| Thyroarytenoid (TA) / Vocalis | Inner thyroid cartilage → vocal process and lateral surface of arytenoid; medial fibers = vocalis muscle | Shortens and relaxes the vocal cord; the vocalis (medial belly) is the body of the true vocal cord | RLN |
| Cricothyroid (CT) | Anterolateral cricoid → inferior thyroid lamina and inferior cornu | Elongates and tenses the vocal cord (raises pitch); the only intrinsic muscle accessible externally | eSLN |
Coding Pearl:
Unilateral RLN injury (e.g., after thyroidectomy, anterior cervical spine surgery, or thoracic surgery) paralyzes all ipsilateral intrinsic muscles except the cricothyroid, resulting in a paramedian cord position. The cricothyroid remains functional because it is supplied by the eSLN. This is why patients with unilateral RLN injury still have some degree of vocal cord tension and residual (if abnormal) phonation.
Extrinsic Muscles of the Larynx
These muscles connect the larynx to surrounding structures and control its vertical position in the neck.
Suprahyoid muscles (elevate the larynx — important in swallowing):
- Digastric, mylohyoid, geniohyoid, stylohyoid
Infrahyoid / Strap muscles (depress the larynx):
- Sternohyoid, sternothyroid, thyrohyoid, omohyoid
Laryngeal Membranes & Ligaments
| Structure | Location & Description | Clinical Importance |
|---|---|---|
| Thyrohyoid membrane | Connects the superior thyroid cartilage to the hyoid bone; the internal branch of the SLN and superior laryngeal artery pierce it laterally | Palpated during surgical approaches; landmark for SLN nerve block injection |
| Cricothyroid membrane (CTM) | Connects the inferior thyroid cartilage to the superior cricoid cartilage; avascular in the midline superior half | Site of emergency cricothyrotomy; landmark for needle decompression of the airway; CPT 31600 (tracheostomy, planned) vs. cricothyrotomy |
| Cricotracheal ligament | Connects inferior cricoid cartilage to first tracheal ring | Defines the laryngotracheal junction; incised during cricotracheal resection |
| Quadrangular membrane | Internal fibrous membrane from the epiglottis to the arytenoid; inferior free edge = false vocal cord (ventricular ligament) | Defines the lateral wall of the laryngeal vestibule |
| Conus elasticus | Fibroelastic membrane; base attaches to the cricoid; superior free edges form the vocal ligaments | The vocal ligament is the critical deep structure preserved during phonomicrosurgery |
| Vocal ligament | Superior free edge of the conus elasticus; extends from the anterior commissure tendon to the vocal process of the arytenoid | Must be identified and preserved during Reinke’s space procedures to maintain voice quality |
Innervation of the Larynx
The larynx is innervated by branches of the vagus nerve (CN X) via two primary nerves:
Superior Laryngeal Nerve (SLN)
Arises from the inferior ganglion of the vagus nerve, descends medial to the carotid artery, and divides at the level of the hyoid:
- Internal branch (iSLN) — purely sensory; pierces the thyrohyoid membrane with the superior laryngeal artery; provides sensation to the supraglottis and epiglottis above the vocal cords; also carries afferent fibers for the cough reflex
- External branch (eSLN) — motor; runs along the inferior pharyngeal constrictor and innervates the cricothyroid muscle; vulnerable during thyroidectomy (Cernea classification describes its anatomical variants near the superior thyroid artery)
Tip
Injury to the eSLN causes loss of high-pitch phonation and easy vocal fatigue — a particular concern for professional voice users (singers, public speakers).
Recurrent Laryngeal Nerve (RLN)
The RLN is the primary motor nerve of the larynx. Its course differs by side:
- Right RLN — loops under the right subclavian artery in the thorax, ascends in the tracheoesophageal groove
- Left RLN — has a longer course, loops under the aortic arch at the ligamentum arteriosum, ascends in the tracheoesophageal groove
The RLN enters the larynx posterior to the cricothyroid joint and innervates all intrinsic muscles except the cricothyroid. It also carries sensory fibers for the subglottic mucosa.
Sites of RLN injury relevant to coding:
| Etiology | ICD-10-CM | RVU / DRG Context |
|---|---|---|
| Thyroidectomy complication | J38.01 + T81.89XA (complication) | May drive higher complexity DRG |
| Thoracic aortic aneurysm compression | J38.01 + I71.2 | Cardiothoracic DRG may be principal |
| Lung cancer compression (left RLN) | J38.01 + C34.xx | Malignancy DRG drives assignment |
| Idiopathic (viral?) | J38.01 | ENT DRG |
| Post-anterior cervical spine surgery | J38.01 + T84.xx complication code | Orthopedic complication context |
Vasculature of the Larynx
Arterial Supply
| Vessel | Origin | Territory |
|---|---|---|
| Superior laryngeal artery | Superior thyroid artery (branch of external carotid) | Supraglottis and upper glottis; accompanies iSLN through thyrohyoid membrane |
| Inferior laryngeal artery | Inferior thyroid artery (branch of thyrocervical trunk from subclavian) | Subglottis and lower posterior larynx; accompanies RLN |
| Cricothyroid artery | Superior thyroid artery | Anterior cricothyroid membrane — surgically important; can bleed during cricothyrotomy if not in the midline inferior half |
Venous Drainage
Mirrors arterial supply — superior laryngeal veins drain to the internal jugular via the superior thyroid vein; inferior laryngeal veins drain to the brachiocephalic via the inferior thyroid venous plexus.
Lymphatic Drainage — Oncologically Critical
| Subsite | Lymphatic Drainage | Clinical Implication |
|---|---|---|
| supraglottis | Bilateral to levels II, III (upper and mid jugular chain) via the preepiglottic space and thyrohyoid membrane | High nodal metastasis rate; bilateral neck dissection often required |
| glottis | Sparse intrinsic lymphatics; minimal drainage to levels II-IV | Low N0→N+ conversion rate for early glottic cancer |
| Subglottis | To levels III, IV, VI (paratracheal/pretracheal nodes) | Subglottic tumors can spread to the central compartment and mediastinum |
Coding relevance:
Neck dissection codes (CPT 38700-38724) and their pairing with laryngectomy codes are driven by extent of lymphadenectomy, which is in turn driven by subsite and nodal metastasis patterns.
Pre-epiglottic Space & Paraglottic Space
Two anatomical compartments of surgical and staging importance:
Pre-epiglottic Space (PES)
- A fat-filled compartment anterior to the epiglottis, superior to the thyrohyoid membrane, and posterior to the thyroid cartilage
- Bounded superiorly by the hyoepiglottic ligament and inferiorly by the thyroepiglottic ligament
- Tumor invasion of the PES (via the foramina of the epiglottis or the preepiglottic fat) upgrades a supraglottic cancer to T3 in AJCC staging
- ICD-10-CM does not code the PES separately, but the T-stage drives specificity in documentation
Paraglottic Space (PGS)
- A bilateral fat-filled space lateral to the quadrangular membrane and conus elasticus, medial to the thyroid lamina
- Provides a corridor for submucosal tumor spread between subsites (supraglottis ↔ glottis ↔ subglottis)
- Paraglottic space invasion is a criterion for T3 staging of laryngeal cancer
- The PGS contains the thyroarytenoid muscle — vocal cord fixation (T3 disease) is often due to thyroarytenoid involvement
Anterior Commissure — Surgical & Staging Significance
The anterior commissure is the point where both true vocal cords converge and attach to the inner surface of the thyroid cartilage via Broyles’ ligament. This ligament is a direct fibrous connection between the vocal ligament and the thyroid perichondrium — it represents an area where the natural barrier between the mucosa and the cartilage is absent or very thin.
Significance:
- Anterior commissure involvement by glottic cancer carries a higher risk of thyroid cartilage invasion because of Broyles’ ligament
- Anterior commissure lesions are more difficult to achieve adequate margins with transoral laser microsurgery
- Radiation treatment planning must account for the anterior commissure as a potential failure site
- Endoscopically, the anterior commissure is the most challenging area to visualize; adequate suspension and patient positioning are critical during direct laryngoscopy
Laryngeal Spaces Visible at Endoscopy
During direct or flexible laryngoscopy, the following landmarks should be systematically examined and documented (essential for operative note accuracy and coding):
| Endoscopic Structure | Location | What to Document |
|---|---|---|
| Vallecula | Space between tongue base and lingual epiglottis | Foreign body, lesion, pooling of secretions |
| Lingual (anterior) surface of epiglottis | Faces the tongue base | Mucosal integrity, lesions, vallecular extension |
| Laryngeal (posterior) surface of epiglottis | Faces the laryngeal inlet | Edema, erythema, lesion |
| Aryepiglottic folds | Lateral walls of laryngeal inlet | Lesion, edema, fixation |
| Piriform sinuses | Bilateral recesses lateral to aryepiglottic folds | Foreign body, tumor, pooling (hypopharynx, not larynx proper) |
| False vocal cords (ventricular folds) | Supraglottic, above the ventricles | Hyperfunction, lesion, erythema |
| Laryngeal ventricles | Recesses between false and true cords | Saccular cyst, laryngocele |
| True vocal cords | Glottic level | Lesion, leukoplakia, erythema, mobility, mucosal wave |
| Anterior commissure | Anterior junction of both true cords | Lesion, webbing |
| Posterior commissure / interarytenoid area | Between arytenoids | Granuloma, pachydermia (contact mucositis from GERD), lesion |
| Subglottis | Below the vocal cords | Stenosis, lesion, tracheal rings visible |
Glottic Gap Patterns and Their Significance
The configuration of the glottis at rest and with phonation provides diagnostic clues:
| Pattern | Appearance | Common Etiology |
|---|---|---|
| Normal | Symmetric triangular opening (posterior glottic chink at rest, full closure with phonation) | No pathology |
| Posterior glottic gap | Persistent posterior opening during phonation | Mild presbylarynx, posterior glottic scar |
| Spindle-shaped gap | Fusiform midcord gap during phonation | Vocal cord atrophy, presbylarynx |
| Unilateral bowing | One cord fails to reach midline | Unilateral paresis or paralysis |
| Hourglass gap | Bilateral midcord defect | Bilateral sulcus vocalis |
| Complete glottic incompetence | Wide-open glottis during attempted phonation | Bilateral paralysis, severe atrophy |
TNM Staging Framework for Laryngeal Cancer (AJCC 8th Edition)
Glottic
| Stage | Criteria |
|---|---|
| T1a | Limited to one vocal cord, normal mobility |
| T1b | Involves both vocal cords, normal mobility |
| T2 | Extends to supraglottis or subglottis; impaired mobility |
| T3 | Cord fixation; invasion of paraglottic space, inner cortex of thyroid cartilage, or pre-epiglottic space |
| T4a | Outer thyroid cartilage, trachea, thyroid gland, esophagus, or soft tissues of neck |
| T4b | Prevertebral space, encases carotid, or invades mediastinal structures |
Supraglottic
| Stage | Criteria |
|---|---|
| T1 | Limited to one subsite, normal cord mobility |
| T2 | Invades mucosa of adjacent subsites, no cord fixation |
| T3 | Cord fixation, invasion of postcricoid area, pre-epiglottic space, paraglottic space, minor thyroid cartilage erosion |
| T4a | Outer thyroid cartilage, trachea, deep tongue muscles, thyroid, esophagus |
| T4b | Same as glottic T4b |
Subglottic
| Stage | Criteria |
|---|---|
| T1 | Limited to the subglottis |
| T2 | Extends to vocal cord(s), normal or impaired mobility |
| T3 | Cord fixation |
| T4a/T4b | Same pattern as above |
Pediatric Laryngeal Anatomy — Key Differences
Relevant to coding newborn laryngoscopy (CPT 31520 vs. 31525) and pediatric airway management:
| Feature | Pediatric | Adult |
|---|---|---|
| Position | Higher (C3-C4 at birth) | Lower (C4-C6 at maturity) |
| Shape | Funnel-shaped (narrowest at subglottis/cricoid) | Cylindrical |
| Narrowest point | Subglottis (cricoid ring) | Glottis |
| Epiglottis shape | Omega (Ω) shaped, softer, more floppy | Leaf-shaped, firmer |
| Arytenoids | Proportionally larger, more prominent | Proportionally smaller |
| Vocal cords | More horizontal, shorter | More angled, longer |
Coding relevance:
The distinction between newborn (31520) and non-newborn (31525) laryngoscopy reflects genuine anatomical and technical differences in instrumentation, airway management, and procedural risk — not merely age-based billing categories.
Common Pathologies by Subsite — Quick Reference
| Pathology | Primary Subsite | ICD-10-CM | CPT Procedure |
|---|---|---|---|
| Vocal cord polyp | Glottis | J38.1 | 31540 or 31541 |
| Vocal cord nodules | Glottis | J38.2 | 31512 or 31545 |
| Reinke’s edema / polypoid corditis | Glottis (Reinke’s space) | J38.3 | 31545 / 31546 |
| Leukoplakia / dysplasia | Glottis | J38.3 | 31535 + pathology |
| Glottic carcinoma | Glottis | C32.0 | 31541 or total laryngectomy |
| Supraglottic carcinoma | Supraglottis | C32.1 | 31540 or supraglottic laryngectomy |
| Subglottic stenosis | Subglottis | J38.6 | 31528 / 31529 / open reconstruction |
| Laryngeal papillomatosis (RRP) | Multi-subsite | D14.1 | 31572 (laser) or 31540 |
| Vocal cord paralysis | Glottis / RLN | J38.01 / J38.02 | 31570 / 31571 (injection); 31560 (arytenoidectomy) |
| Subglottic hemangioma (pediatric) | Subglottis | D18.09 | 31572 (laser) |
| Contact granuloma | Posterior glottis / interarytenoid | J38.7 | 31540 or medical management |
| Laryngocele | Ventricle / supraglottis | J38.7 | 31540 or external excision |
| epiglottitis / supraglottitis | Supraglottis | J04.30 / J04.31 | 31525 (evaluation); airway intervention if needed |
Related Concepts & Cross-References
- 31525 — Direct Laryngoscopy, Diagnostic
- 31520 — Direct Laryngoscopy, Newborn
- 31535 — Direct Laryngoscopy with Biopsy
- 31545 — Microlaryngoscopy with Submucosal Resection
- 31575 — Flexible Fiberoptic Laryngoscopy
- C32.0 — Malignant Neoplasm of Glottis
- C32.1 — Malignant Neoplasm of Supraglottis
- J38.1 — Polyp of Vocal Cord
- J38.01 — Unilateral Vocal Cord Paralysis
- J38.6 — Stenosis of Larynx