Comprehensive Anatomy and Physiology Guide for Medical Coding Professionals
🫀 Introduction to Anatomy and Physiology in Medical Coding
https://en.wikipedia.org/wiki/Outline_of_human_anatomy#General_anatomy
The foundation of accurate, compliant, and efficient medical coding rests upon a profound understanding of human anatomy and physiology. Anatomy focuses on the structural organization of the human body, detailing the exact location, composition, and physical relationships of organs, tissues, and systems. Physiology explores the mechanical, physical, and biochemical functions of these structures, explaining how they interact to sustain life, repair injury, and maintain homeostasis. The intersection of these two disciplines forms the bedrock of modern medical documentation and health information management.

Medical coding is the precise transformation of healthcare diagnoses, procedures, medical services, and equipment into universal medical alphanumeric codes. The diagnoses and procedure codes are abstracted from complex medical record documentation, such as transcriptions of physician notes, operative reports, laboratory results, and radiologic imaging interpretations. Medical coding professionals serve a critical function in the healthcare revenue cycle; they help ensure that these alphanumeric codes are applied correctly during the medical billing process, which includes abstracting the information from documentation, assigning the appropriate codes, and creating a claim to be paid by insurance carriers. This practice has deep historical roots, deriving from public bills of mortality posted in London in the 18th century, where correlating data allowed doctors to determine the cause of a cholera epidemic. Today, the data derived from medical codes is utilized not only for provider reimbursement but also to determine utilization rates, manage actuarial risk, identify resource allocation, build actuarial tables, and support global public health initiatives.
For professionals tasked with translating these complex medical records, mastering anatomy and physiology is not optional; it is an absolute necessity. Medical coders must interpret detailed physician documentation and correlate them with highly specific codes from the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), the Current Procedural Terminology (CPT) manual, and the Healthcare Common Procedure Coding System (HCPCS). Furthermore, the ICD-10 Procedure Coding System (ICD-10-PCS) requires exact anatomical localization to assign the correct body part and approach characters for inpatient procedures. An exhaustive understanding of anatomy and physiology reduces coding errors, mitigates the risk of costly insurance claim denials, ensures proper reimbursement, and supports the integrity of global healthcare data. Without this knowledge, coders risk misclassifying conditions, which can potentially jeopardize a patient’s access to necessary care or trigger audits for non-compliance.
The Language of Medicine: Medical Terminology and Word Construction

To effectively navigate the complexities of anatomy, physiology, and procedural documentation, medical coders must be fluent in medical terminology. Health care professionals use long, unfamiliar medical terms to describe conditions that under normal circumstances would take several words to describe. Medical terminology facilitates effective and efficient communication by conveying a great quantity of information with precision in the fewest number of words.
Most medical terms are constructed using three primary word components: a prefix, a root word (or combining form), and a suffix. If all three word parts are present in medical terminology, they will invariably appear in the order of prefix, followed by the root word, and concluding with the suffix. The root word provides the core meaning and generally refers to the body part or organ system in question. The prefix appears at the beginning of the medical term and adds modifying information, such as spatial location, severity, or quantity. Finally, the suffix is positioned at the end of the term and usually indicates a specific procedure, condition, disease, or theory.
When defining an unfamiliar medical term, coders are trained to start the definition with the suffix, then move to the prefix, and finally the root. For example, in the term “antibacterial,” the suffix “-al” means “pertaining to,” the prefix “anti-” means “against,” and the root “bacteri-” means “bacteria”—yielding a definition of something pertaining to protecting against bacteria. Similarly, the term “tonsillitis” utilizes the root “tonsil” and the suffix “-itis” (inflammation), clearly denoting an inflammation of the tonsils. Understanding these components allows a coder to dissect and comprehend highly complex operative reports, even when encountering an obscure or highly specialized surgical term for the first time.
Essential Prefixes, Suffixes, and Root Words
The table below outlines common prefixes and suffixes that medical coders encounter daily when abstracting documentation for ICD-10-CM and CPT code assignment.
| Word Part | Type | Meaning | Clinical Example and Application |
|---|---|---|---|
| a-, an- | Prefix | Lack of, without, not | Analgesic: Medication administered without causing pain, or to relieve pain. |
| dys- | Prefix | Bad, painful, difficult | Dysrhythmia: An abnormal physiological rhythm, commonly referring to cardiac conduction issues. |
| hyper- | Prefix | Above, excessive, beyond | Hypertension: High blood pressure, an excessive force against arterial walls. |
| hypo- | Prefix | Below, beneath, deficient | Hypoglycemia: A deficient or low level of sugar in the blood. |
| -itis | Suffix | Inflammation | Bronchitis: Inflammation of the bronchial airways. |
| -ectomy | Suffix | Excision, surgical removal | Cholecystectomy: The surgical removal of the gallbladder. |
| -plasty | Suffix | Surgical repair | Rhinoplasty: The surgical repair or reconstruction of the nose. |
| -lysis | Suffix | Breakdown or destruction | Hemolysis: The destruction or breakdown of red blood cells. |
| -genesis | Suffix | Formation or origin | Pathogenesis: The origin and development of a disease process. |
| -cyte | Suffix | Cell | Erythrocyte: A mature red blood cell. |
| -blast | Suffix | Immature cell | Osteoblast: A bone-forming immature cell. |
| -clast | Suffix | Destroying cell | Osteoclast: A bone-resorbing or destroying cell. |
| -ism | Suffix | Condition or theory | Dysmorphism: A condition of anatomical malformation. |
Mastering root words specific to body systems is equally critical. These roots often utilize a combining vowel (usually an “o”) to connect with suffixes that begin with a consonant, creating a “combining form”. The table below categorizes vital anatomical root words by body system.
| Combining Form | Body System / Organ | Clinical Terminology Example |
|---|---|---|
| Pulmon/o, Pneum/o | Respiratory (Lung, air) | Pneumonia: Inflammation of lung tissue. |
| Bronch/o | Respiratory (Bronchus) | Bronchitis: Inflammation of the bronchi. |
| Laryng/o | Respiratory (Larynx) | Laryngoscopy: Visual examination of the larynx. |
| Cardi/o | Cardiovascular (Heart) | Cardiovascular: Pertaining to the heart and blood vessels. |
| Gastr/o | Digestive (Stomach) | Gastritis: Inflammation of the stomach lining. |
| Hepat/o | Digestive (Liver) | Hepatoblastoma: A malignant liver tumor. |
| Enter/o | Digestive (Intestine) | Enteropathy: Disease of the intestine. |
| Cholecyst/o | Digestive (Gallbladder) | Cholecystectomy: Removal of the gallbladder. |
| Nephr/o | Urinary (Kidney) | Nephrotoxic: Harmful or destructive to the kidneys. |
| Oste/o | Musculoskeletal (Bone) | Osteoporosis: Condition of bone loss and porosity. |
| Arthr/o | Musculoskeletal (Joint) | Arthritis: Inflammation of the joints. |
| My/o | Musculoskeletal (Muscle) | Myopathy: Disease affecting muscle tissue. |
| Chondr/o | Musculoskeletal (Cartilage) | Chondromalacia: Softening of the cartilage. |
| Neur/o | Nervous (Nerve) | Neuroblast: An immature nerve cell. |
| Dermat/o | Integumentary (Skin) | Dermatitis: Inflammation of the skin. |
| Opt/o | Special Senses (Eye) | Optometrist: Specialist who measures eye function. |
Anatomical Directional Terms and Body Planes
Medical documentation heavily utilizes standardized anatomical terminology to describe the precise location of injuries, lesions, and surgical interventions. The beginning of an anatomy and physiology course can feel like wading through a sea of confusing new terminology, but a visual and conceptual grasp of anatomical planes, positions, and directional terms keeps coders afloat. Mastery of these spatial relationships is essential for assigning accurate diagnosis codes and applying the correct CPT modifiers for laterality (left versus right) or specific anatomical sites.
A description of any region or part of the body in a specific stance is predicated on the “anatomical position”. In the standard anatomical position, the human body is upright, directly facing the observer, with feet flat and directed forward. The upper limbs are situated at the body’s sides with the palms facing forward. When a patient is lying face up, they are in the supine position; conversely, lying face down is the prone position. Directional terms are words used to describe the position of one body structure relative to another, and they are frequently grouped in pairs that possess opposite meanings.
Standard Directional Terms
Coders must commit these terms to memory to avoid confusion when studying or describing the locations of particular body parts within operative and imaging reports.
| Directional Term | Definition and Spatial Relationship | Anatomical Example |
|---|---|---|
| Anterior (Ventral) | Describes the front or the direction toward the front of the body. | The kneecap (patella) is located on the anterior side of the leg. |
| Posterior (Dorsal) | Describes the back or the direction toward the back of the body. | The shoulder blades (scapulae) are located on the posterior side of the body. |
| Superior (Cranial) | Describes a position above or higher than another part of the body proper; toward the head end. | The hand is part of the superior extremity relative to the foot. |
| Inferior (Caudal) | Describes a position below or lower than another part of the body proper; away from the head or near the tail (coccyx). | The foot is part of the inferior extremity. |
| Medial | Describes the middle or the direction toward the midline of the body. | The hallux (big toe) is the medial toe, located at the medial side of the foot. |
| Lateral | Describes the side or the direction toward the side of the body, away from the midline. | The thumb is lateral to the index finger in the standard anatomical position. |
| Proximal | Describes a position in a limb that is nearer to the point of attachment or the trunk of the body. | The brachium (upper arm) is proximal to the antebrachium (forearm). |
| Distal | Describes a position in a limb that is farther from the point of attachment or the trunk of the body. | The crus (lower leg) is distal to the femur (thigh bone). |
| Superficial | Describes a position closer to the surface of the body. | The skin is superficial to the underlying skeletal bones. |
| Deep | Describes a position farther from the surface of the body, situated internally. | The brain is deep to the skull. |
Anatomical Body Planes
Medical imaging (such as Magnetic Resonance Imaging and Computed Tomography scans) and complex surgical approaches are often described using body planes. Planes are imaginary flat surfaces that divide the human body into specific sections, allowing clinicians and radiologists to view internal structures from various standardized angles.
| Anatomical Plane | Division Mechanism and Description | Clinical Imaging Context |
|---|---|---|
| Sagittal Plane (Lateral Plane) | A vertical plane running from front to back that divides the body or an organ vertically into right and left sides. | If this vertical plane runs directly down the absolute middle of the body, it is specifically termed the midsagittal or median plane, dividing the body into equal right and left halves. |
| Frontal Plane (Coronal Plane) | A vertical plane running from side to side that divides the body or an organ into an anterior (front) portion and a posterior (rear) portion. | Often referred to as a coronal plane, this view is critical for assessing structures that span the width of the body, such as the lungs or the pelvic girdle. |
| Transverse Plane (Axial or Horizontal Plane) | A horizontal plane that divides the body or organ horizontally into superior (upper) and inferior (lower) portions. | Transverse planes produce imaging slices referred to as cross sections, which are the standard presentation for CT scans traversing the abdomen or thorax. |
Global Architecture of Medical Coding Systems
Understanding the human body requires parallel knowledge of how the predominant medical coding systems are structured to capture anatomical data. The global standard for diagnostic reporting is the ICD-10-CM, while procedural coding in outpatient and physician settings relies on the CPT code set. Furthermore, inpatient facility procedures require the use of the ICD-10-PCS, which introduces an entirely different alphanumeric architecture based heavily on anatomical approaches and root operations.
ICD-10-CM Chapter Organization
The 10th edition of the International Classification of Diseases (ICD-10) is a medical coding system designed by the World Health Organization (WHO) to catalog health conditions by mapping complex diseases to broader morbidities. The U.S. version, ICD-10-CM, was created by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). It is used for medical claim reporting in all healthcare settings to represent conditions, diseases, related health problems, abnormal findings, signs and symptoms, injuries, external causes, and social circumstances. While CPT codes depict the services provided to the patient, ICD-10-CM codes depict the patient’s diagnoses that justify those services as medically necessary. The ICD-10-CM manual is intricately structured by body systems and disease etiologies, making an understanding of anatomical chapters critical for rapid code retrieval and validation.
Certain conditions have both an underlying etiology and multiple body system manifestations due to that underlying etiology. For such conditions, the ICD-10-CM utilizes a coding convention that requires the underlying condition to be sequenced first, followed by the manifestation code. Wherever such a combination exists, there is a “use additional code” note at the etiology code, and a “code first” note at the manifestation code, dictating the proper sequencing order.
| ICD-10-CM Chapter Range | Associated Body System or Disease Category |
|---|---|
| A00-B99 (Chapter 1) | Certain Infectious and Parasitic Diseases |
| C00-D49 (Chapter 2) | Neoplasms |
| D50-D89 (Chapter 3) | Diseases of the Blood and Blood-Forming Organs, and Certain Disorders of the Immune Mechanism |
| E00-E89 (Chapter 4) | Endocrine, Nutritional, and Metabolic Diseases |
| F01-F99 (Chapter 5) | Mental, Behavioral, and Neurodevelopmental Disorders |
| G00-G99 (Chapter 6) | Diseases of the Nervous System |
| H00-H59 (Chapter 7) | Diseases of the Eye and Adnexa |
| H60-H95 (Chapter 8) | Diseases of the Ear and Mastoid Process |
| I00-I99 (Chapter 9) | Diseases of the Circulatory System |
| J00-J99 (Chapter 10) | Diseases of the Respiratory System |
| K00-K95 (Chapter 11) | Diseases of the Digestive System |
| L00-L99 (Chapter 12) | Diseases of the Skin and Subcutaneous Tissue |
| M00-M99 (Chapter 13) | Diseases of the Musculoskeletal System and Connective Tissue |
| N00-N99 (Chapter 14) | Diseases of the Genitourinary System |
CPT Surgical Section Organization
The CPT code set, managed by the American Medical Association (AMA), uses five-digit numeric or alphanumeric codes to designate procedures and services. Category I codes correspond to a procedure or service and range from 00100 to 99499, ordered into sub-categories based heavily on procedure type and anatomy. Within the Surgery section (10004-69990), the structure progresses generally from the integumentary system down through the musculoskeletal, respiratory, cardiovascular, digestive, urinary, and reproductive systems. These categories are divided into broad procedures (such as General, Excision, or Repair) and further separated into specific code ranges designating the exact type of procedure completed and the anatomical location.
| CPT Code Range | Surgical Body System Section |
|---|---|
| 10040-19499 | Integumentary System (Skin, Subcutaneous Tissue, Accessory Structures, Nails, Breast) |
| 20000-29999 | Musculoskeletal System (Neck/Thorax, Spine, Upper/Lower Extremities, Pelvis, Hip Joint) |
| 30000-32999 | Respiratory System (Nose, Accessory Sinuses, Larynx, Trachea, Bronchi, Lungs, Pleura) |
| 33010-37799 | Cardiovascular System (Heart & Pericardium, Arteries & Veins, Cardiac Valves) |
| 38100-38999 | Lymphatic System (Spleen, Lymph Nodes) |
| 40000 Series | Digestive System Procedures |
| 50000 Series | Urinary System, Male Genital System, Female Genital System, Maternity Care |
| 60000 Series | Endocrine System and Nervous System Procedures |
| 69000 Series | Eye and Ocular Adnexa, Auditory System |
ICD-10-PCS Inpatient Procedural Architecture
For inpatient hospital settings, the ICD-10 Procedure Coding System (ICD-10-PCS) is employed. Every ICD-10-PCS code is exactly seven characters long, and each character represents a distinct aspect of the procedure. Character 1 defines the Section (e.g., 0 for Medical and Surgical), Character 2 defines the Body System (e.g., 00 for Central Nervous System, 0B for Respiratory, 0D for Gastrointestinal), and Character 3 identifies the Root Operation.
The Root Operation describes the objective of the procedure. For example, the physical eradication of all or a portion of a body part by the direct use of energy, force, or a destructive agent is assigned the root operation “Destruction” (Value 075). Cutting out or off, without replacement, a portion of a body part is “Excision” (Value 07B). Taking out or off a device from a body part and putting back an identical or similar device without cutting or puncturing the skin is “Change” (Value 072). Taking or letting out fluids and/or gases from a body part is “Drainage” (Value 079).
Character 4 defines the specific Body Part, detailing the exact anatomical site where the procedure is performed (e.g., distinguishing between the Right Lobe of the Liver, the Gallbladder, or the Common Bile Duct). Character 5 defines the Approach, which is the technique used to reach the site of the procedure. A thorough understanding of anatomical approaches is vital for accurate PCS coding.
| ICD-10-PCS Approach | Clinical Definition and Anatomical Mechanism |
|---|---|
| Open | Cutting through the skin or mucous membrane and any other body layers necessary to expose the site of the procedure (e.g., Abdominal hysterectomy). |
| Percutaneous | Entry, by puncture or minor incision, of instrumentation through the skin or mucous membrane and any other body layers necessary to reach the site of the procedure (e.g., Needle biopsy of the liver). |
| Percutaneous Endoscopic | Entry, by puncture or minor incision, of instrumentation through the skin or mucous membrane and any other body layers necessary to reach and visualize the site of the procedure (e.g., Arthroscopy). |
| Via Natural or Artificial Opening | Approaches through an existing orifice without puncturing the skin, traversing natural anatomical pathways. |
Detailed Anatomical System Analysis
With the foundational terminology and coding architectures established, a detailed analysis of the major human body systems provides the necessary context for accurate clinical abstracting.
1. The Integumentary System
The integumentary system is a complex and highly specialized structure that serves as the body’s first line of defense. It comprises the skin, hair, nails, sebaceous (oil) glands, sweat glands, and various specialized cellular components.
Anatomy and Physiology
The skin is composed of three distinct tissue layers, each with specific physiological roles that dictate coding implications.
-
Epidermis: The outermost layer is made of closely packed epithelial cells, including squamous cells, basal cells, and melanocytes. The epidermis provides a waterproof barrier, creates human skin tone through melanin production, and continually regenerates.
-
Dermis: Situated beneath the epidermis, the dermis is composed of dense, irregular connective tissue. This robust layer houses critical structures such as blood vessels, hair follicles, sweat glands, and nerve endings. The dermis provides elasticity, tensile strength, and thermoregulation through the dilation and constriction of its vascular network.
-
Subcutaneous Tissue (Hypodermis): The deepest layer lies beneath the dermis and is composed primarily of loose connective and fatty (adipose) tissues. It serves as a vital thermal insulator and physical shock absorber for underlying organs and muscles.
The overarching functions of the integumentary system include protection against environmental pathogens, sensation (processing touch, pain, and temperature variations), thermoregulation, and complex wound healing processes.

Clinical Coding Applications
A profound understanding of the integumentary layers is vital for selecting CPT codes, particularly for excisions, skin grafts, and wound debridement. Debridement codes (CPT 11042-11047) are assigned based strictly on the specific depth of the tissue removed and the total surface area measured in square centimeters (sq cm). For example, debridement of subcutaneous tissue corresponds to CPT 11042 for the first 20 sq cm, while +11045 is used as an add-on code for each additional 20 sq cm. If a debridement extends deeper into the muscle layer—such as for a patient with gangrene—the coder must assign 11043 for the primary area and +11046 for additional areas. In severe cases, such as a foot ulcer requiring debridement down to the bone, the coder utilizes 11044 and +11047. The mathematical combination of surface areas from different anatomical sites is a common challenge that requires precise reading of the operative report.
In the ICD-10-CM, conditions are coded based on location, severity, and the specific layer affected. Coders encounter terms like dermatitis and eczema (L20-L30), psoriasis and papulosquamous disorders (L40-L45), urticaria and erythema (L50-L54), and diseases of the hair, such as alopecia (L60-L75). Skin lesions—whether they present as macules, papules, nodules, or ulcers—require precise anatomical identification. A cellulitis diagnosis implies a bacterial skin infection causing redness and swelling, while a melanoma originates from the melanocytes in the epidermis. Furthermore, coders must trust the ICD-10-CM Index; for instance, the term “skin tag” directs the coder to L91.8, even though the tabular code description does not explicitly include the term “skin tag”.
2. The Musculoskeletal System
The musculoskeletal system provides the rigid framework for the human body, enabling structural support, physical protection of internal organs, and voluntary movement.
Anatomy and Physiology
This system is composed of an intricate network of connective tissue, muscles, ligaments, and bones.
-
Bones: Major skeletal landmarks include the femur (thigh), tibia (shin), humerus (upper arm), radius and ulna (forearm), vertebrae (spine), and the calcaneus (heel bone). Bones store essential minerals and house the bone marrow, which is crucial for hematopoiesis (the production of blood cells).
-
Joints: Articulations such as the shoulder, elbow, hip, knee, and vertebral joints facilitate movement.
-
Muscles: Skeletal muscles, including the deltoid, biceps, quadriceps, and hamstrings, act upon the bones to produce mechanical movement.
-
Ligaments and Tendons: Ligaments (e.g., the Anterior Cruciate Ligament [ACL] and Posterior Cruciate Ligament [PCL]) connect bone to bone, providing crucial joint stability. Tendons (e.g., the Achilles tendon) connect muscle to bone, translating the contractile force of the muscle into skeletal motion.
Clinical Coding Applications
Musculoskeletal coding is highly nuanced due to the vast array of bones and joints. In ICD-10-CM (Chapter 13, M00-M99), conditions like osteoarthritis (M15-M19), spondylopathies (M45-M49), muscle disorders (M60-M63), and other soft tissue disorders (M70-M79) require high diagnostic specificity. For instance, a diagnosis of rheumatoid myopathy with rheumatoid arthritis maps to M05.4. Trauma coding demands exact anatomical precision; an injury such as a calcaneus fracture must be classified clearly. Under the highly specific ICD-10-CM system, a displaced intraarticular fracture of the right calcaneus, initial encounter for a closed fracture, maps to S92.061A.
In the CPT manual (20000-29999), musculoskeletal procedures are categorized generally by anatomical region (e.g., Neck, Spine, Upper Arm, Pelvis, Hip Joint) and subsequently by the type of procedure, such as an incision, excision, or repair. Whether a coder is assigning codes for simple fracture care, complex total joint replacements, or arthroscopic tendon repairs, a detailed understanding of the system’s structural geometry is vital to prevent claim denials.
3. The Respiratory System
The respiratory system facilitates the critical physiological process of respiration, exchanging gases by delivering oxygen to the bloodstream and expelling carbon dioxide from the body.
Anatomy and Physiology
The system is divided into upper and lower respiratory tracts, featuring highly specialized structures :
-
Airways: The trachea (windpipe) serves as the main conduit for air, bifurcating into the right and left bronchi, which further branch into progressively smaller bronchioles.
-
Lungs: The lungs consist of lobes (three on the right side, two on the left) and contain millions of microscopic, grape-like air sacs called alveoli. The alveoli are enveloped by a capillary network where the actual physiological gas exchange occurs. The lungs are encased in a protective double-layered membrane known as the pleura.
-
Musculature: The diaphragm serves as the primary muscle of respiration, contracting to create a negative pressure vacuum in the thoracic cavity. It is supported by accessory muscles such as the intercostals (between the ribs) and scalene muscles in the neck.

Clinical Coding Applications
Respiratory diagnoses are consolidated under ICD-10-CM Chapter 10 (J00-J99). The clinical specificity required for these codes demands a solid anatomical foundation. For instance, acute bronchitis (J20.-) must be coded to the specific viral or bacterial agent when documented; J20.0 indicates Mycoplasma, J20.1 indicates streptococcus, and J20.5 indicates respiratory syncytial virus (RSV). Furthermore, conditions like asthma are classified by clinical severity. Intermittent asthma is clinically defined as occurring less than or equal to two times per week. Coders must also heed explicit “use additional code” instructions in this chapter to report associated tobacco exposure (Z77.22), tobacco dependence (F17.-), or a history of tobacco use (Z87.891).
Procedurally, respiratory CPT codes (30000-32999) cover surgical and diagnostic interventions progressing from the nose, accessory sinuses, and larynx down to the trachea, bronchi, lungs, and pleura. Coders must differentiate between procedures based on the depth of the airway accessed and the anatomical structures visualized. For example, a coder must distinguish the work involved in a routine intubation, a diagnostic bronchoscopy, or a therapeutic thoracentesis (the removal of fluid from the pleural space).
4. The Cardiovascular System
The cardiovascular system operates continuously to transport oxygen, vital nutrients, hormones, and cellular waste products throughout the body via a vast network of blood vessels driven by the heart. If this supply is reduced or cut off for even a few minutes, affected cells will die, making diseases of this system acutely life-threatening.

Anatomy and Physiology
The heart serves as the central muscular pump, structurally divided into four distinct chambers: the right and left atria (upper receiving chambers) and the right and left ventricles (lower pumping chambers).
-
Valves: Directional blood flow is strictly maintained by four valves. The tricuspid and mitral (bicuspid) valves separate the atria from the ventricles, while the pulmonary and aortic semilunar valves regulate flow out of the ventricles.
-
Major Vessels: Oxygenated blood exits the heart via the aorta, while the pulmonary trunk routes deoxygenated blood to the lungs. The superior and inferior vena cava return deoxygenated blood from the systemic circulation back to the heart. The heart muscle itself relies on the coronary arteries for its own blood supply.
-
Conduction System: The heart’s electrical rhythm—the heartbeat—is generated and regulated autonomously by the Sinoatrial (SA) node, the Atrioventricular (AV) node, and the bundle of His.
-
Tissue Layers: The heart wall comprises three layers: the endocardium (inner lining), myocardium (the thick muscular layer), and epicardium (the outer layer).

Clinical Coding Applications
Cardiovascular conditions dominate many inpatient and outpatient medical records, making anatomical mastery imperative. Coders must identify distinct pathologies such as myocardial infarctions (MI), heart valve disorders, and arrhythmias. In ICD-10-CM, complex combination codes exist for conditions like atherosclerotic heart disease accompanied by angina pectoris; these codes require the coder to differentiate between blockages in native vessels versus blockages in a previously placed coronary bypass graft. Furthermore, coding guidelines for a myocardial infarction require a strict understanding of the healing timeframe, which is defined as 28 days. Any subsequent MI occurring within that 28-day window requires specific sequencing and code assignment.
For surgical procedures (CPT 33010-37799), anatomical landmarks dictate code selection. The category is broadly divided into the Heart & Pericardium and Arteries & Veins, with subcategories dedicated to specific valves like the Aortic and Mitral valves. Surgical procedures such as percutaneous transluminal coronary angioplasty (PTCA), stent placement, coronary artery bypass grafting (CABG), and pacemaker insertions (which relate directly to the SA/AV node conduction system) rely heavily on precise anatomical documentation of the vessels and chambers involved.
5. The Digestive System
The digestive (gastrointestinal or GI) system is responsible for the mechanical and chemical breakdown of food, the absorption of essential nutrients into the bloodstream, and the excretion of solid waste.
Anatomy and Physiology
The GI tract is a continuous muscular tube extending from the mouth to the anus, supported by vital accessory organs that facilitate digestion:

-
Upper GI Tract: The mouth initiates mechanical digestion, aided by saliva enzymes. The esophagus then transports the food bolus to the stomach. The stomach utilizes strong acids and enzymes to break down food into a semi-fluid mass called chyme.
-
Lower GI Tract: The small intestine absorbs the vast majority of nutrients into the bloodstream via microscopic projections called villi. The large intestine (colon) subsequently absorbs water and electrolytes, forming solid waste.
-
Accessory Organs: The liver, gallbladder, and pancreas are crucial for digestion. The liver produces bile, which is stored in the gallbladder, while the pancreas secretes digestive enzymes and hormones.
-
Structural Layers and Sphincters: The walls of the GI tract consist of four layers: the mucosa, submucosa, muscularis, and serosa. Key circular muscles called sphincters, such as the lower esophageal sphincter and the pyloric sphincter, regulate the passage of contents between organs and prevent backflow.

Clinical Coding Applications
ICD-10-CM maps digestive diseases to Chapter 11 (K00-K95). Coders encounter diagnoses ranging from upper GI issues like gastroesophageal reflux disease (GERD) and peptic ulcers, to lower GI and accessory conditions like Crohn’s disease, irritable bowel syndrome (IBS), and pancreatitis.
In the CPT manual, the 40000 series is dedicated to digestive system procedures. A coder’s anatomical knowledge is frequently tested when distinguishing between the extent of endoscopic procedures. For example, knowing the exact starting and ending points of an esophagogastroduodenoscopy (EGD) versus a colonoscopy is critical. An EGD visualizes the esophagus, stomach, and the proximal duodenum, while a colonoscopy examines the entire colon from the rectum to the cecum. Accurately coding bariatric surgeries, gastrectomies, and gallbladder removals requires a deep understanding of the surgical approach and the specific GI tract layers involved.
6. The Urinary System
The urinary system functions as the body’s primary filtration and excretory mechanism, regulating fluid volume, electrolyte balance, and the elimination of liquid waste, primarily urea.
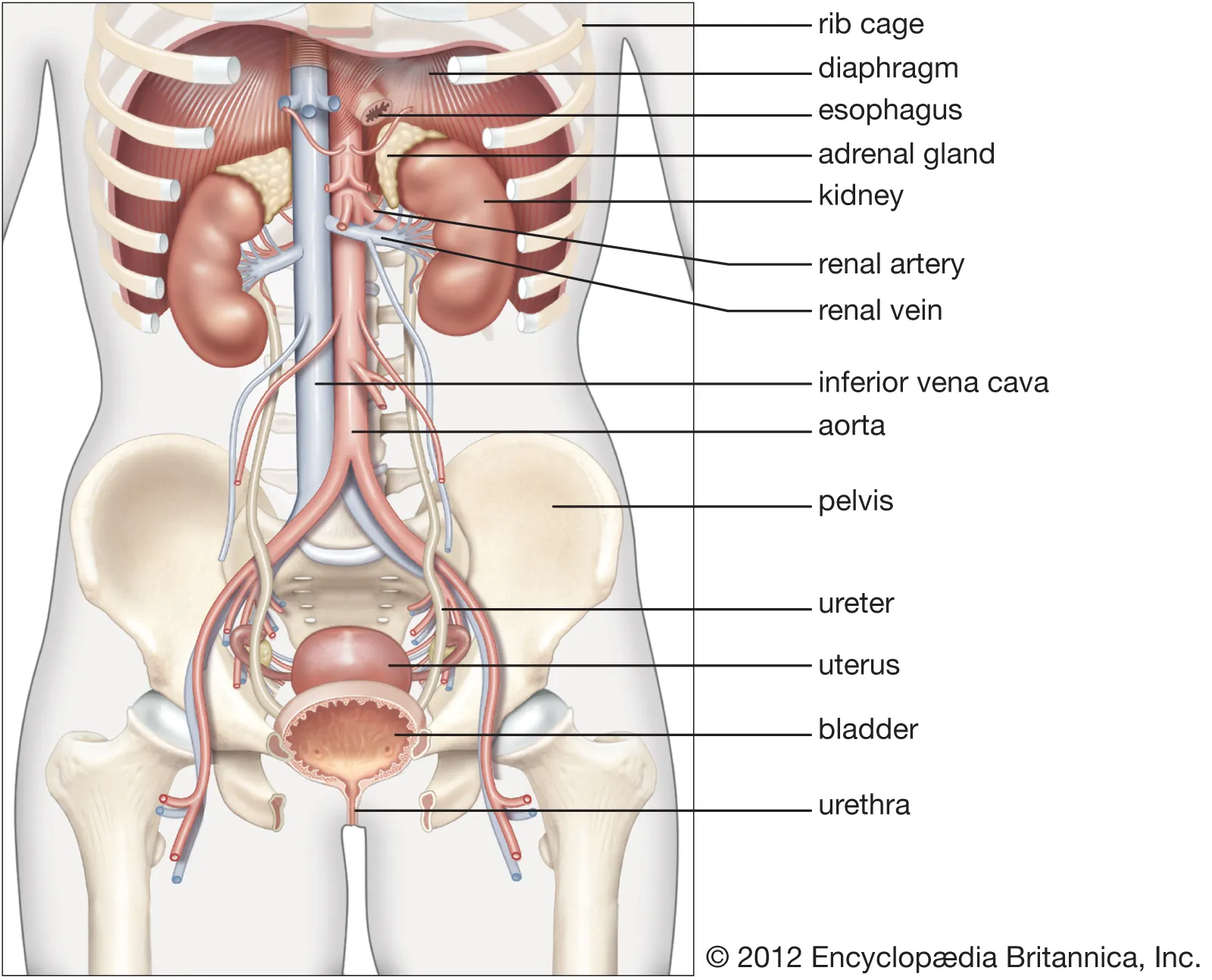
Anatomy and Physiology
The primary structures of the urinary system include:
-
Kidneys: Two bean-shaped organs responsible for blood filtration. Structurally, they consist of an outer cortex, an inner medulla, and millions of functional filtration units called nephrons.
-
Ureters: Muscular tubes that transport urine from the renal pelvis of the kidneys down to the bladder using peristaltic movements.
-
Bladder: A hollow, muscular sac that stores urine. Anatomical landmarks within the bladder are highly specific. The bladder wall contains the detrusor muscle. The dome refers to the roof of the bladder, while the posterior wall refers to the back. A critical landmark is the trigone—a smooth, triangle-shaped region located near the junction of the urethra and the bladder base.
-
Urethra: The terminal passage through which urine is excreted from the body. Two circular sphincter muscles surround the urethra to maintain continence and prevent urine from leaking.

Clinical Coding Applications
Genitourinary diseases are classified in ICD-10-CM under Chapter 14 (N00-N99). Common diagnoses include urinary tract infections (UTIs), kidney stones (nephrolithiasis), renal failure, and structural abnormalities.
For procedural coding, the CPT 50000 series covers the urinary system. The specific anatomical site dictates the code selection. When coding a cystoscopy (the visual examination of the bladder), the documentation will frequently reference landmarks such as the trigone, the lateral walls, or the dome to describe the exact location of a biopsy or tumor fulguration. Coders must understand these landmarks to accurately report the size and location of bladder tumors. Similarly, procedures like lithotripsy (stone crushing) or a nephrectomy (kidney removal) require strict anatomical verification against the operative report to ensure the correct code is billed.
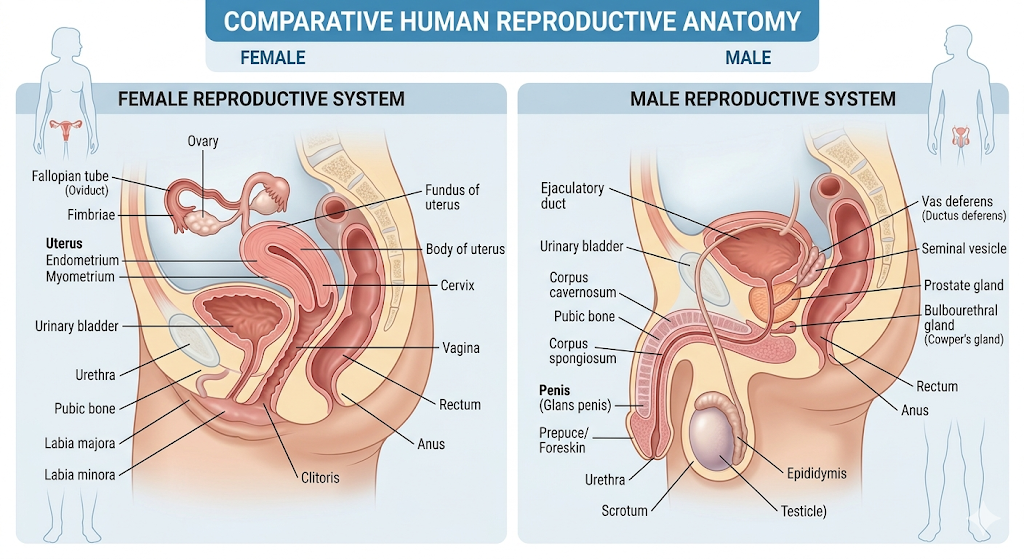
7. The Reproductive Systems
The male and female reproductive systems are specialized for procreation and are heavily influenced by hormonal regulation. Medical coding separates these systems due to their distinct anatomical and procedural requirements.
Anatomy and Physiology: Female Reproductive System
The female system comprises both internal organs and external genitalia.
-
External Genitalia (Vulva): The vulva is an area lying posterior to the mons pubis (a pad of fat located over the pubic bone). It includes the labia majora (large, hair-covered outer folds that protect other organs) and the labia minora (smaller, thinner, pigmented inner folds). The superior, anterior portions of the labia minora converge to encircle the clitoris, a highly sensitive erectile organ. The vaginal opening (introitus) and the external urethral meatus are located within the vestibule. The hymen is a piece of tissue partially covering the vaginal opening. The perineum is the physical area located between the vulva and the anus.
-
Internal Organs: Includes the muscular vagina, the cervix (the neck of the uterus), the uterus (womb), the fallopian tubes, and the ovaries.

Anatomy and Physiology: Male Reproductive System
The male system focuses on the production and delivery of sperm and includes the penis, testis (which produce sperm and testosterone), epididymis (where sperm mature), the protective scrotum, the vas deferens, spermatic cord, seminal vesicles, and the prostate gland, which contributes fluid to the ejaculate.
Clinical Coding Applications
The CPT manual divides reproductive and maternity services meticulously based on these general anatomical areas.
-
Male Genital System (CPT 54000-55899): Covers procedures on the penis, testis, epididymis, tunica vaginalis, scrotum, vas deferens, spermatic cord, seminal vesicles, and prostate. Procedures range from circumcisions to complex prostatectomies.
-
Female Genital System (CPT 56405-58999): Covers procedures categorized by anatomical site, starting externally at the vulva and perineum, and moving internally to the vagina, cervix, uterus, oviducts (fallopian tubes), and ovaries. This section also encompasses codes for In Vitro Fertilization.
-
Maternity Care and Delivery (CPT 59000-59899): These five-digit codes correspond to services provided in uncomplicated maternity cases, specifically covering antepartum care, delivery services, and postpartum care. Notably, medical complications of pregnancy are not coded in this range but are listed in the Medicine or Evaluation & Management sections, while surgical complications of pregnancy are included in specific Surgery sections.
8. The Endocrine System
The endocrine system works synergistically with the nervous system to maintain homeostasis. Rather than utilizing fast-acting electrical impulses, it relies on chemical messengers (hormones) secreted directly into the bloodstream.
Anatomy and Physiology
This system is characterized by ductless glands distributed throughout the body. Major structures include the hypothalamus, pituitary, thyroid, parathyroid, and adrenal glands, as well as the endocrine portion of the pancreas (the islets of Langerhans), ovaries, and testes. Hormones secreted by these glands regulate metabolism, physical growth, sexual function, and sleep cycles. For instance, the hypothalamus initiates physiological changes (like hunger, thirst sensations, or heart rate modifications) based on mental states or systemic needs.

Clinical Coding Applications
ICD-10-CM Chapter 4 (E00-E89) encompasses Endocrine, Nutritional, and Metabolic diseases. Coding these conditions requires careful attention to causality, specificity, and detailed documentation. Endocrine disorders occur when hormone levels are abnormally high or low, which could stem from genetic factors, tumors, or the physical removal of a gland. A condition like myxedema coma (E03.5) denotes a severe, naturally underactive thyroid. However, if the hypothyroidism is a direct result of the surgical removal of thyroid tissue, it requires a distinct, specific code (E89.0, Postprocedural hypothyroidism). Other critical codes include nondiabetic hypoglycemic coma (E15), Waterhouse-Friderichsen syndrome involving adrenal gland failure (A39.1), and Waldenstrom macroglobulinemia (C88.0).
From a procedural standpoint, endocrinology utilizes a specific mix of CPT codes spanning multiple sections :
-
Evaluation and Management (E/M): Codes 99201-99205 (New patient visits) and 99211-99215 (Established patient visits) are heavily utilized to manage complex metabolic disorders like diabetes. Consultation codes (99241-99245) are applied when a physician requests an expert opinion from an endocrinologist; documentation must clearly support the rationale for the consultation and the complexity of medical decision-making.
-
Laboratory Diagnostics (80047-89398): Specific quantitative laboratory measurements are crucial for diagnosing endocrine disorders. For example, thyroid function is assessed via specific tests for TSH (84443), Free T4 (84436), and Free T3 (84439). Insulin levels (83036), quantitative blood glucose (82947), and glucose tolerance tests (82950) are essential for diabetes management and assessment of pancreatic function.
-
Procedures: While less common than lab testing, procedures like fine needle aspiration biopsies of glands (e.g., thyroid biopsy CPT 10004), thyroid ultrasounds (76536), and hormone therapy injections (CPT 96372) demand strict anatomical documentation to support medical necessity and prevent claim denials.

9. The Nervous System
The nervous system acts as the body’s primary control and communication network, maintaining rapid homeostasis through the transmission of electrical impulses.
Anatomy and Physiology
The system is anatomically and functionally divided into two primary subdivisions:
-
Central Nervous System (CNS): Comprising the brain and the spinal cord, this subdivision serves as the primary integrative control center.
-
Peripheral Nervous System (PNS): Comprising all other neural elements, including the cranial nerves extending from the brain and the spinal nerves extending from the spinal cord.
The PNS is further subdivided based on functional directionality:
-
Afferent (Sensory) Neurons: Transmit impulses from peripheral sensory receptors toward the CNS.
-
Efferent (Motor) Neurons: Transmit commands from the CNS outward to muscles and glands.

The Efferent division is split into the Somatic nervous system (managing voluntary skeletal muscle control) and the Autonomic nervous system (managing automatic, involuntary control of cardiac/smooth muscle and glandular secretions). The Autonomic system is kept in balance by the Sympathetic (“fight or flight” response, utilizing epinephrine to increase heart rate and blood pressure) and Parasympathetic (“rest and digest” system, conserving energy and stimulating digestion) divisions.
Tip
At the cellular level, the nervous system consists of impulse-conducting Neurons and supporting Neuroglia (Glial cells). Glial cells insulate and support nervous tissue; CNS glial cells include astrocytes, oligodendrocytes, ependymal cells, and microglia, while PNS glial cells include Schwann cells.
Clinical Coding Applications
Nervous system diseases are reported via ICD-10-CM Chapter 6 (G00-G99). The specificity in this chapter is intense. For example, coding Parkinson’s disease requires coders to distinguish the presence of dyskinesia and fluctuations; G20.A1 indicates Parkinson’s without dyskinesia and without mention of fluctuations, while G20.B2 indicates the presence of both dyskinesia and fluctuations. Neuropathies (such as G60.9, Hereditary and idiopathic neuropathy) and autonomic system degenerations (G90.3) are similarly coded with high specificity.

Procedural coding for the nervous system utilizes the 60000 series in the Surgery section of the CPT manual. Procedures range from peripheral nerve blocks and epidural injections for pain management to complex craniotomies and spinal laminectomies. Coders must thoroughly understand nerve distributions and spinal cord segmental levels (cervical, thoracic, lumbar) to accurately assign codes and append modifiers indicating laterality.
10. The Special Senses (Eye and Ear)
Though technically specialized extensions of the nervous system responsible for sensory input, the ocular (eyes) and auditory (ears) structures are clinically separated in coding manuals due to their highly unique pathologies and specialized procedural interventions.
Anatomy and Physiology
- Eye and Ocular Adnexa: The visual system includes the eyeball, optic nerve, extraocular muscles, eyelids, conjunctiva, and the lacrimal (tear) apparatus.
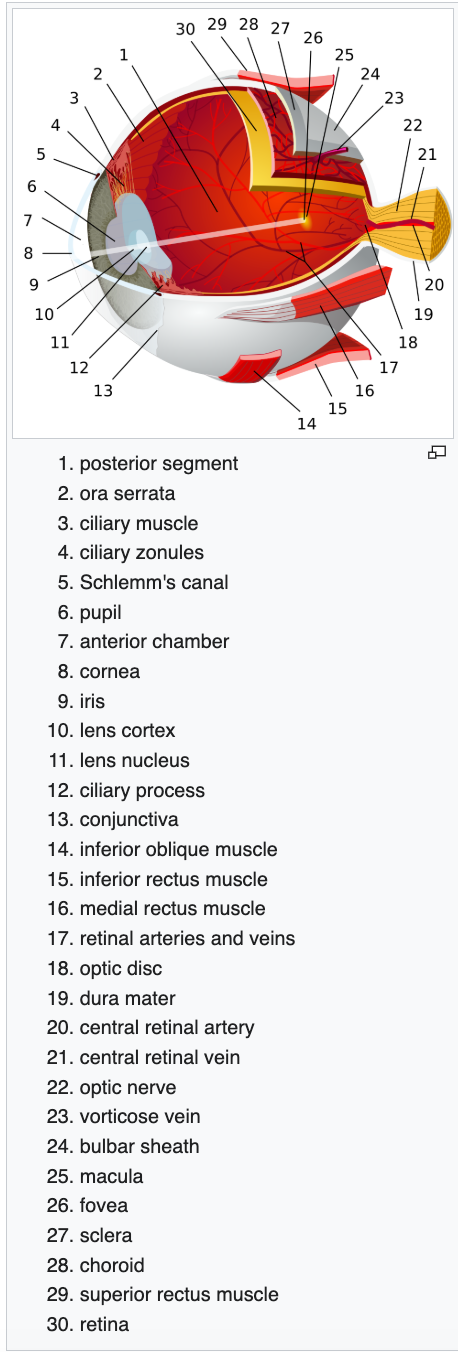
- Ear and Mastoid Process: The auditory and vestibular system is divided into three parts: the external ear, the middle ear (containing the tympanic membrane and the three ossicles), and the inner ear (housing the cochlea for hearing and the vestibular system for spatial balance).

Clinical Coding Applications
ICD-10-CM isolates these organs into distinct, highly specialized chapters: Chapter 7 (H00-H59) is dedicated to diseases of the eye and adnexa, and Chapter 8 (H60-H95) covers the ear and mastoid process. The anatomical specificity required here is immense, as nearly all codes require laterality. For example, a diagnosis of otitis media must specify whether it affects the right ear, left ear, or is bilateral, and whether the effusion is serous, suppurative, or allergic in nature. CPT coding in the 69000 series involves precise anatomical identification for procedures such as cataract extractions, tympanostomies (ear tube placements), and audiometric testing.
11. Hematopoietic, Lymphatic, and Immune Systems
These interconnected systems are responsible for circulating vital fluids, defending against pathogenic invasions, and maintaining fluid balance in the interstitial tissue spaces.

Anatomy and Physiology
- Hematopoietic System (Blood): Blood is a specialized liquid connective tissue comprising plasma (the liquid matrix) and formed cellular elements.
| Blood Component | Clinical Function and Physiological Details |
|---|---|
| Erythrocytes (Red Blood Cells - RBCs) | Responsible for oxygen transport using Hemoglobin (Hgb). They have a 120-day lifespan and are produced in the bone marrow. Anemia is defined clinically as a reduction in functional RBCs or hemoglobin content. |
| Leukocytes (White Blood Cells - WBCs) | The defenders of the immune system. A normal count ranges from 3.5 to 10.5 billion cells/L. They are categorized as granulocytes (Neutrophils 60-70%, Eosinophils 4-6%, Basophils 1%) and agranulocytes (Lymphocytes 20-25%, Monocytes 3-8%). |
| Thrombocytes (Platelets - PLT) | Essential for hemostasis, they prevent blood loss by adhering to damaged vessels and initiating the clotting cascade, which forms fibrin strands. A normal count is 150-450 billion/L. |
-
Lymphatic System: This system consists of lymphatic vessels, lymph nodes, the spleen, thymus, and tonsils. Because blood pressure forces fluid to leak from capillaries into the interstitial space (the spaces between individual cells), the lymphatic system is required to maintain fluid balance. It absorbs approximately 3 liters of excess interstitial fluid daily, returning it to the bloodstream as lymph. A failure in this drainage mechanism—such as a blockage by cancer cells or destruction by injury—results in protein-rich fluid accumulation, clinically referred to as lymphedema. The spleen also serves lymphatic functions by filtering old RBCs and pathogens.
-
Immune System: The immune system employs both non-specific innate defenses and specific adaptive immunity. Innate defense includes the skin, mucous membranes, inflammation (characterized by heat, redness, pain, and swelling caused by histamine release), and fever. The adaptive immune response requires exposure to a pathogen and utilizes Cell-mediated immunity (where T-cells attack pathogens directly) and Antibody-mediated immunity (where B-cells produce specific antibodies). These antibodies are Immunoglobulins (e.g., IgG fights bacteria/viruses, IgA protects mucous membranes, IgM causes RBC clumping, and IgE stimulates allergic reactions).

Clinical Coding Applications
Blood and immune disorders are classified under ICD-10-CM Chapter 3 (D50-D89). Conditions range from various anemias and coagulation defects to complex immunodeficiencies, such as defects in the complement system (D84.1) or cryoglobulinemia (D89.1).
CPT coding for these systems involves extensive laboratory testing. Coders must frequently bill for panels such as the Complete Blood Count (CBC), CBC with differential, Hematocrit (Hct), Hemoglobin (Hgb), PT/PTT (to assess clotting time), INR (for monitoring anticoagulation therapy), and ESR (sedimentation rate, associated with systemic inflammation). The surgical aspect of the Lymphatic system is found in the 38100-38999 CPT range, encompassing excisions, repairs, and biopsies of the spleen and various lymphatic channels.
Regions
- The cranial region includes the upper part of the head while the
- facial region includes the lower half of the head beginning below the ears.
- The forehead is referred to as the frontal region.
- The eyes are referred to as the orbital or ocular region.
- The cheeks are referred to as the buccal region.
- The ears are referred to as the auricle or otic region.
- The nose is referred to as the nasal region.
- The mouth is referred to as the oral region.
- The chin is referred to as the mental region.
- The neck is referred to as the cervical region.
The trunk of the body contains, from superior to inferior,
- the thoracic region encompassing the chest
- the mammary region encompassing each breast
- the sternal region encompassing the sternum
- the abdominal region encompassing the stomach area
- the umbilical region is located around the navel
- the coxal region (hip region) encompassing the lateral (side) of hips
- the pubic region encompassing the area above the genitals.
The pelvis and legs contain, from superior to inferior,
- the inguinal or groin region between the thigh and the abdomen,
- the pubic region surrounding the genitals,
- the femoral region encompassing the thighs,
- the patellar region encompassing the front of the knee,
- the crural region encompassing the lower leg, between the knee and ankle,
- the fibular region encompassing the outside of the lower leg,
- the tarsal region encompassing the ankle,
- the pedal region encompassing the foot
- the digital/phalangeal region encompassing the toes.
- The great toe is referred to as the hallux.
The regions of the upper limbs, from superior to inferior, are
- the axillary region encompassing the armpit,
- the brachial region encompassing the upper arm,
- the antecubital region encompassing the front of the elbow,
- the antebrachial region encompassing the forearm,
- the carpal region encompassing the wrist,
- the palmar region encompassing the palm,
- the digital/phalangeal region encompassing the fingers.
- The thumb is referred to as the pollex.
The posterior view contains, from superior to inferior,
- the cervical region encompassing the neck,
- the scapular region encompassing the scapulae and the area around,
- the dorsal region encompassing the upper back
- the lumbar region encompassing the lower back.
- the sacral region occurring at the end of the spine, directly above the buttocks.
The regions of the back of the arms, from superior to inferior, include
- the cervical region encompassing the neck,
- the acromial region encompassing the shoulder,
- the brachial region encompassing the upper arm,
- the olecranal region encompassing the back of the elbow,
- the antebrachial region encompasses the forearm, front and back
- and the manual or manus region encompassing the back of the hand.
The posterior regions of the legs, from superior to inferior, include
- the gluteal region encompassing the buttocks,
- the femoral region encompassing the thigh,
- the popliteal region encompassing the back of the knee,
- the sural region encompassing the back of the lower leg,
- the calcaneal region encompassing the heel,
- the plantar region encompassing the sole of the foot.
Some regions are combined into larger regions. These include the trunk, which is a combination of the thoracic, mammary, abdominal, navel, and coxal regions. The cephalic region is a combination of all of the head regions. The upper limb region is a combination of all of the arm regions. The lower limb region is a combination of all of the leg regions.
Conclusion
The intersection of human anatomy, physiology, and medical coding represents a complex but highly structured domain. The ongoing evolution of classification systems, particularly the transition to the highly granular ICD-10-CM and the intricately structured ICD-10-PCS, necessitates an uncompromising standard of anatomical literacy among health information professionals. Whether differentiating between the muscular and subcutaneous layers for a surgical debridement, identifying the specific coronary artery targeted during an angioplasty, or understanding the endocrine feedback loops prompting a diagnostic laboratory panel, the coder’s knowledge directly dictates the accuracy of the clinical narrative. By mastering the foundational terminology, spatial body planes, and the intricate physiological processes of every major body system, medical coders ensure the seamless translation of patient care into standardized data. This data, in turn, acts as the lifeblood of modern healthcare, driving accurate reimbursement, shaping institutional policy, and empowering global health analytics.