levator-palpebr--aesuperior- — Muscle that elevates and retracts the upper eyelid (“the lifting muscle of the superior eyelid”)
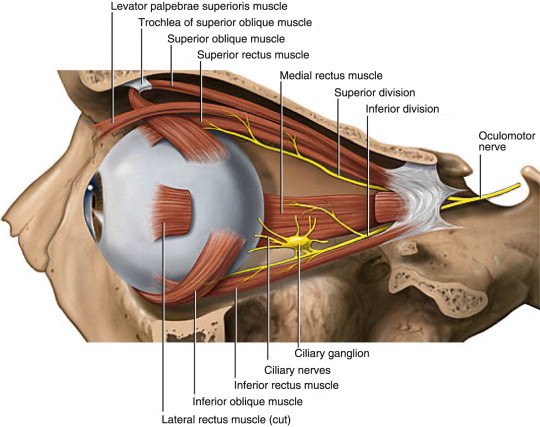
The levator palpebrae superioris (LPS) is a triangular skeletal muscle in the orbit that originates from the periosteum of the lesser wing of the sphenoid bone (superior to the optic foramen), travels anteriorly above the superior rectus muscle, and fans out into the levator aponeurosis, which inserts onto the skin of the upper eyelid and the superior tarsal plate; it is the primary elevator of the upper eyelid and functions under both voluntary and involuntary control; its smooth muscle counterpart, the superior tarsal muscle (Müller’s muscle), arises from its undersurface and is innervated by postganglionic sympathetic fibers from the superior cervical ganglion; damage to either structure or their innervation results in ptosis (drooping of the upper eyelid).
Classical latin New Latin anatomical terminology:
• Levator-: Latin levare = “to lift, to raise” + -tor (agent noun) = “one who raises.”
• Palpebr-: Latin palpebra = “eyelid” (possibly from palpare = “to touch gently, to stroke”).
• Superior-: Latin superus = “above, upper,” comparative form = “higher of the two.”
• Literal: “The raiser of the upper eyelid” — a precise anatomical description of function.
Anatomical Profile
Feature
Detail
Origin
Periosteum of lesser wing of sphenoid bone, superior to optic foramen
Insertion
Skin of upper eyelid; superior tarsal plate (via levator aponeurosis)
Innervation
Superior division of CN III (oculomotor nerve)
Blood Supply
Muscular branches of ophthalmic artery; supraorbital artery
extraocular muscles: The 7 extrinsic eye muscles, of which LPS is one.
superior rectus: Runs inferior to LPS in orbit; shares fascial connections.
Clinical Details
Assessment: Margin-reflex distance 1 (MRD1) — normal ≥3.5 mm; levator function measured by excursion (normal ≥12 mm); fatigue test for myasthenia gravis.
Symptoms of dysfunction: Drooping upper lid, visual field obstruction superiorly, head tilt/chin-up posturing, amblyopia risk in children.
Surgical repair: Approach and CPT code selection depend on levator function — good function (≥5 mm) → levator resection (67903/67904); poor function → frontalis sling (67901/67902); Müller’s muscle resection (67908) for Horner’s ptosis.
Botox use: CN injection into LPS intentionally induces temporary ptosis to protect the cornea in facial nerve palsy.
One-Sentence Summary
The levator palpebrae superioris (Latin: “raiser of the upper eyelid”), innervated by the superior division of CN III, is the primary elevator of the upper lid via its aponeurosis and superior tarsal muscle; dysfunction at any level — neurogenic (H02.433), myogenic (H02.421), or aponeurotic (H02.401) — produces ptosis, repaired surgically via levator resection (CPT 67903/67904) or frontalis sling (CPT 67901/67902).